Cancer has traditionally been the diagnosis people fear most. But is dying from cancer so much worse than the alternatives? Anna Wagstaff tries to make sense of an emotive discussion that all started with a post on the BMJ blog.
“How do you want to die? You must think about it.” This is the message that Richard Smith, former editor of the British Medical Journal, wanted to get across in a short piece he posted on the BMJ blog on New Year’s Eve 2013.
By New Year’s Day, his post was being reported all over the UK media, and during the following week it spread across the world, triggering an avalanche of online discussion as it went.
Why such a response? Because given a choice, Smith says he would choose to die from cancer. He titled his blogpost “Dying of cancer is the best death”.
“There are … essentially four ways to die,” wrote Smith. “Sudden death; the long, slow death of dementia; the up and down death of organ failure, where it’s hard to identify the final going down, tempting doctors to go on treating too long; and death from cancer, where you may bang along for a long time but go down usually in weeks.”
Sudden death is typically the favourite choice when the question is put to audiences, says Smith. But while it may work well for the deceased, “ [it] may be very tough on those around you.” Dementia may be the most awful, “as you are slowly erased”. Death from organ failure – lung, heart or kidney – on the other hand, involves too much time spent in hospital “in the hands of doctors”.
The advantage of death from cancer, says Smith, is that while it is possible to live with incurable disease for a long time, the dying process happens relatively fast, yet slow enough to give time for yourself and those around you to prepare for your death and say goodbye. Smith finishes with a caution to “stay away from over-ambitious oncologists” who don’t know when it’s time to stop active treatment and allow the disease to take its course.
Given that cancer has traditionally, across time and across cultures, been the diagnosis people fear most, the title of the piece was enough to ensure it would be widely circulated. But it was Smith’s description of how those final weeks could be spent that really set the tone of the discussions that erupted on the BMJ and other websites.
Love morphine and whisky
The scenario he painted – “reflecting on life, leaving last messages, visiting special places, listening to favourite music, and preparing, according to your beliefs, to meet your makers or enjoy eternal oblivion” – was one that he himself admitted was “a romantic view of dying”. But “with love, morphine and whisky”, it could be achievable he suggested.
Smith’s blogpost drew a barrage of comments expressing hurt, fury and indignation. People were astounded that their own terrible experiences with cancer could be described in such a glib fashion.
– “Dying a slow death from cancer is a nightmare. There is nothing to romanticize. There is no mellow philosophical self reflection during that time. Instead there is fear, extended grief, hardship, suffering, enormous financial burdens.”
– “Death by cancer HURTS: tumors can gradually cut off your air supply, compress your heart so it can’t beat properly, block your gut so you can’t eat, erode your bones, press on nerves, or destroy bits of your brain so you can’t control your body or think properly.”
– “…Opiates do not control the pain, it is a constant battle between pain, constipation and laxatives and a cocktail of painkillers which do not control all pain.”
– “It took my mother 15 months of ever-increasing pain and physical and mental disability to die from a transitional cell carcinoma in the sinus behind her right eye. No death could have been more cruel.”
– “My father suffered two months of not being able to eat or swallow, which led to him being so weak he could not get out of bed… The cancer also affected his mind so that he was not capable of sorting out his affairs, or even of rational conversation at times. And did we enjoy having this ‘extra’ time seeing him in such distress? Not in the slightest.”
There were many others, however, who wrote in support of Smith’s overall purpose and message, including people who had watched family members die or were themselves diagnosed with incurable cancer.
– “I would take the ‘sudden death’ option myself, but I do understand his point of view that organ failure and dementia REALLY suck, and as an RN [registered nurse] working in long-term care facilities, I see all too many people suffering for years on end with these conditions.”
– “I helped my sisters and brother at my mother’s death, at 96. It was sad of course, and was a long time coming. But compared with my father in law’s death 50 years ago in a car crash, I’d say the hole in our families’ lives were greater following the car crash.”
– “I was diagnosed with cancer and am grateful that I have cancer rather than dementia. It has increased my joy of life as I am now part of the exclusive club of people who truly know that life will end and the only possible insurance is to enjoy the moment.”
– “The clarity of transition for many cancer patients to palliative care whilst clearly distressing does introduce a new if unwelcome certainty. This is what is missing from the experience of the growing population of people who are experiencing ‘progressive dwindling’ from degenerative diseases such as Alzheimer’s.”
– “Provided there are a good amount of painkillers available and, perhaps more importantly, an accepting mindset of the individual… I agree that this is indeed the best way to pass over.”
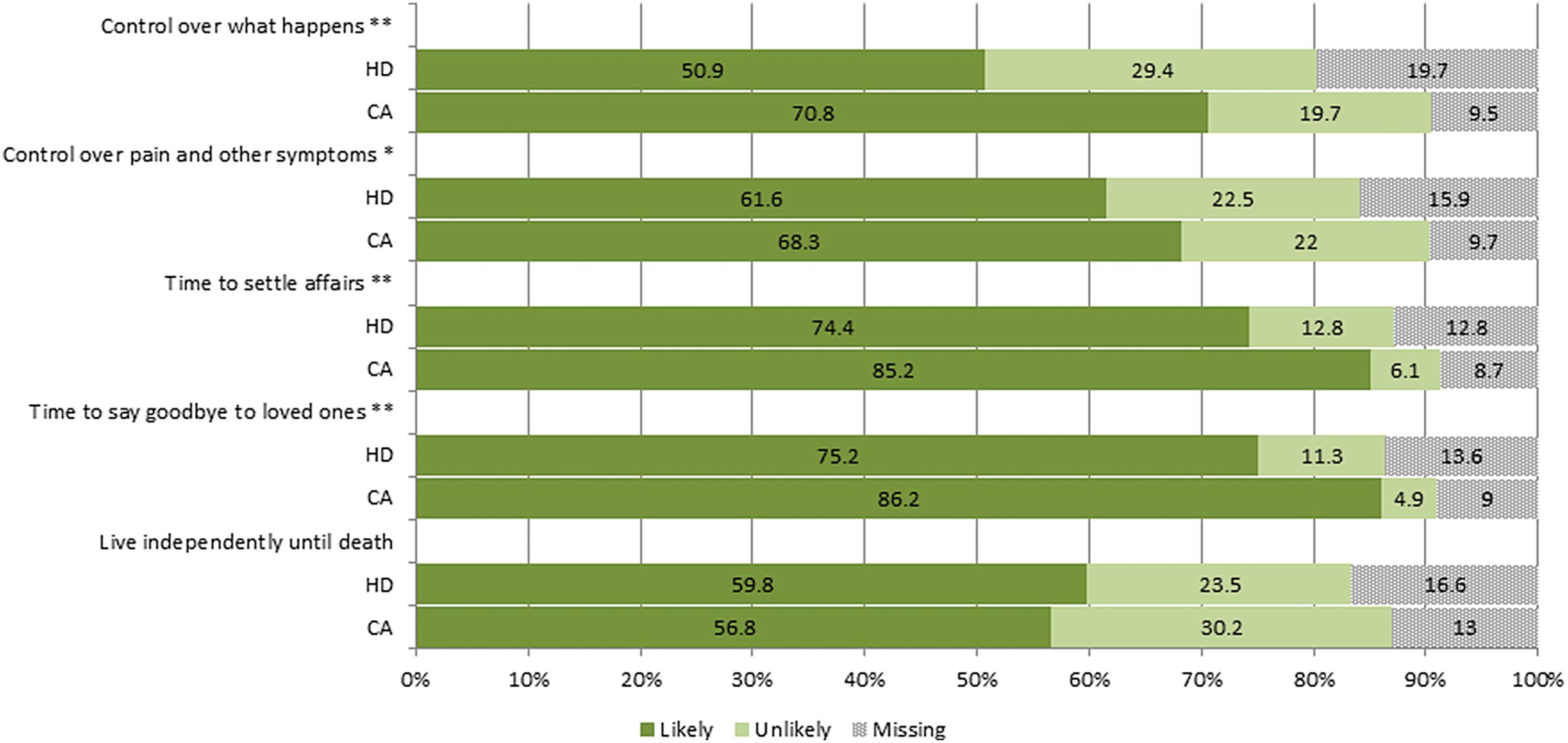
The discussion triggered by Smith’s blogpost prompted Charlotte Vrinten and Jane Wardle, from University College London’s Health Behaviour Research Centre, to find out how the general public rates dying from cancer. Specifically, they wanted to know whether they rate it as better or worse than dying from heart disease, on the basis of five characteristics of ‘a good death’ selected from the end-of-life literature (Eur J Can 2016, 56:172–178).
The five chosen characteristics were:
control over what happens
control over pain/symptoms
time to settle affairs
time to say goodbye and
living independently until death.
Most respondents agreed that four out of five of these “good death” attributes would be more likely with cancer than heart disease, with the exception being living independently until death (see figure).
‘A good death’ : cancer vs heart disease
This survey of public attitudes among middle-aged and older people showed that dying of cancer (CA) was seen as preferable to dying from heart disease (HD) on four of the five attributes of a ‘good death’ they were asked about Source: C Vrinten and J Wardle (2016) Eur J Cancer 56:172–178, republished under a creative commons license *P < 0.01, **P < 0.001 (click to enlarge)
Their study also quoted UK evidence indicating that dying of cancer was associated with better access to palliative care services – a finding that has been reported in other countries.
Why have this conversation?
Arguing the pros and cons of different ways of dying may seem a futile exercise, given that the choice of how we die is rarely ours to make. Even those opting for suicide, whether assisted or otherwise (a fifth way Smith chose not to include), cannot choose the circumstances that led them down that path.
“If you at least think what sort of end would I like… probably the experience is going to be better
than if you try not to think about it at all”
However, as the online discussion in response to Smith’s blogpost shows, it does seem to be effective at encouraging people to overcome our understandable aversion to thinking and talking about the process of dying. This could well pay off when the time comes, Smith told Cancer World.
“We’re all going to die and I think that there is quite convincing evidence that if you at least think what sort of end would I like… where would I like to die, then probably the experience is going to be better than if you try not to think about it at all.”
Referring to his “romantic” description of dying from cancer, he says that this was probably coloured by the experiences of his own parents. His father died a quick and easy death from renal cancer: “He coughed up blood in January and he had a mass on his chest X-ray… He was dead by March 4th. He had a magnificent death. Didn’t have any morphine. Died at home. He was 81. He never thought he’d make it that far.”
His mother, meanwhile, lives in a nursing home and has had no short-term memory for 10 years. “I’m pretty clear about which one I’d choose,” says Smith.
He recognises that many deaths from cancer are more protracted and more painful than his father’s, and that not everyone has reached old age when cancer strikes, or finds it easy to accept that their time has come. And he did issue an apology to the people who had been angered and upset by his post.
But he also points out that most health professionals who commented broadly agreed with his core argument: cancer is largely a disease of old age, and what works with cancer is the timescale. “Although everybody wants a sudden death, most people won’t die that way – probably less than 10% of them. And it may be alright for you but it’s certainly not good for the people around you. Whereas if you die of cancer, you can sort out things, you can say goodbye to people.”
Something to aim for
Carlos Centeno is palliative care specialist based at Navarra University Hospital, in Pamplona, who is leading efforts to map and develop palliative care services across Europe, and has 20 years of experience providing symptom relief for countless patients, particularly during their final months and weeks of life.
He points out that many years before her own death, the founder of the hospice movement Dame Cicely Saunders said that if she could choose what to die of, she would choose cancer. As it turned out, that is what happened – she died of breast cancer in the hospice she had founded, St Christopher’s in London.
“It is very poetic to say I want to die of cancer,
but a cancer that is free of pain, suffering,
deterioration. This is not a cancer”
Centeno is clear, however, that the rose-tinted death we all aspire to is the exception rather than the rule.
“I think that the idea of having time for preparation, a time to say goodbye, to receive love and give love, is the kind of death any of us would choose. We all want this time, without suffering, to do what we want to do. But the problem is we don’t always have this peaceful time. It is very poetic to say I want to die of cancer, but a cancer that is free of pain, free of suffering, free of deterioration, free of complications, free of all that. This is not a cancer. This is a dream.”
Dance of Death, by Frans Francken the Younger, ca. 1635
The physiological process of dying from advanced cancer follows no strict path, he says. “Today I have a patient with kidney cancer who is very short of breath. This is unusual for kidney cancer, but then nothing is typical for kidney cancer. Any cancer can give any symptoms in any place.”
Death, he says, tends to come from multiple problems that feed into one another until it becomes impossible for the body to sustain life. Metastases to the bone, he says, eventually kill because they replace the factory of the blood. But bone metastases tend to happen at the same time as liver metastases, and deteriorating liver function also kills you. Kidney failure is another common cause of death, as the body’s metabolism goes down: “The patient starts with dehydration, and that leads to kidney failure and the patient dies from renal failure. Any possibility can happen in any kind of cancer.”
“Often dying of cancer is very hard,” says Centeno. Nonetheless, he broadly subscribes to Richard Smith’s recipe of love, morphine and whisky. Indeed he flags up the underuse of morphine across Europe as a serious cause of unnecessary suffering in dying patients. “At the end of life, morphine in expert hands is our friend. The family doctor, the general oncologist – not just palliative care specialists – have to be expert in managing this kind of medication,” he says.
He emphasises, too, that despite the suffering from a failing body, sustained emotional and spiritual support can bring something positive to the experience of dying. “If you are receiving this sort of support in your physical deterioration, you can find you are a person with a life that is always preserved for those who are around you – in some way you are experiencing more as a person than ever,” he says.
That’s how it should be anyway.
‘There are other ways to do this’
However, Centeno worries that in practice opportunities to prepare for loss and death are being lost because of our (understandable) reluctance to accept the reality of approaching death, combined with the illusion given by modern medicine that we can somehow postpone our end indefinitely – kick-start hearts, by-pass feeding routes, ‘treat’ terminally resistant cancers.
Like many people both within and outside the medical profession, Centeno – who works in a hospital setting – feels that something about the way we die within modern medicine is wrong, and we need to find better ways to manage our relationship with death and dying.
He contrasts Western attitudes with those he experienced on a recent trip to Uganda, where he spent some time with a community-based palliative care team. The team is part of the pioneering service that has been running in that country for almost 35 years, and has given the country a world ranking of 35 in The Economist’s 2015 Quality of Death Index – above several European countries, and highly impressive given that Uganda ranks 163 on the Human Development Index. The system is designed to deliver support and symptom relief – not least morphine – to people dying in their own homes.
“We have to go back to other ways to do medicine, other ways to do business with death”
“In Uganda people understand that life has a time, and at a certain time you have to go,” says Centeno. “This is a natural process. In our advanced societies, the feeling is that you can buy anything, you have the right to have anything. Something is wrong. We have to go back to other ways to do medicine, other ways to do business with death.”
Can we “go back”? Can countries like Uganda learn to enjoy the benefits of modern medicine without losing their accepting attitude towards death? This is an issue that Seamus O’Mahony, an Irish consultant gastroenterologist tackles in his recently published book The way we die now: We have lost the ability to deal with death.
Ireland, notes O’Mahony, is a country that turned from one of the most religious in Europe to one of the least in the course of a generation; that experienced the 1990’s power rush of economic growth when it seemed money could buy anything, and is now going through a grim period of austerity following the 2008 financial crash.
O’Mahony argues that, having discarded the religious rituals it once relied on to “tame” dying and grieving, society has tried to hand responsibility for delivering “a good death” over to the medical profession – which cannot possibly oblige. He questions in particular the extent to which responsibility for people’s spiritual/existential wellbeing is being brought within the medical sphere. He also echoes the sentiments of many of Richard Smith’s harshest critics, arguing that the concept of death with dignity is itself largely a romantic illusion.
“Having discarded religious rituals,
society has tried to hand responsibility for delivering
‘a good death’ over to the medical profession”
Death, he says, is “an affliction… more marked by pain, fear, boredom and absurdity than by dignity, spirituality and meaning.” People who are dying, he argues, are often “too tired, too spent, to be spiritual” – a sentiment that will no doubt be appreciated by people who feel they are being blamed for not being able to die a more graceful death, or help others to do so.
O’Mahony’s overall message, however, does chime with both Smith and Centeno. We’re doing this wrong. We all need to learn how to deal with death as a natural part of our lives. The only way that will happen is if we overcome our natural resistance and think about it and talk about it.
The rising popularity of events like Death Cafés, where people can gather to have those conversations over tea and cake, may be an early sign of a new readiness to rehabilitate the topic of death and dying into our everyday conversations.
1 Comment on When your time is up. Conversations about dying from cancer
No offense, but taking advice about how to deal with your death from a doctor doesn’t sit well with me. Doctors experience death regularly, to them it’s another day on the job, obviously they’re going to tell you it could be worse and that it’s just death no big deal. They see death a lot different than the normal person does, I bet most lack empathy after a certain amount of years on the job. I’m in Canada where doctors don’t care, maybe it’s different elsewhere. That’s my two cents.







No offense, but taking advice about how to deal with your death from a doctor doesn’t sit well with me. Doctors experience death regularly, to them it’s another day on the job, obviously they’re going to tell you it could be worse and that it’s just death no big deal. They see death a lot different than the normal person does, I bet most lack empathy after a certain amount of years on the job. I’m in Canada where doctors don’t care, maybe it’s different elsewhere. That’s my two cents.