The state of the art on the diagnosis and management of cancer of the pancreas and hepatobiliary system was the focus of the 3rd St Gallen Gastrointestinal Cancer Conference, held earlier this year under the auspices of the EORTC. Jonas Feilchenfeldt reviews the highlights.
This grandround was first presented by Jonas Feilchenfeldt, from the National Center for Cancer Care and Research (NCCCR), Doha, Qatar, as a live webcast for the European School of Oncology. It is edited by Susan Mayor. The webcast of this and other e-sessions can be accessed at e-eso.net.
The St. Gallen International Gastrointestinal Cancer Conference takes place every two years under the auspices of the European Centre for Research and Treatment of Cancer. This year it looked at primary therapy of early GI cancers, with a focus on hepatobiliary and pancreatic cancers. A webcast of the two-day programme can be accessed at www.oncoconferences.ch. What follows are selected highlights of some of the key presentations.
Discriminating pancreatic cystic neoplasms: histopathological and molecular features
Irene Esposito (Essen, Germany) considered how to discriminate between pancreatic cystic neoplasms, drawing on a case series of 788 consecutive pancreatic resections that included 86 patients with cystic lesions of the pancreas (HPB Surgery 2015, doi.org/10.1155/2015/847837). During surgery the group found that 61% had intraductal papillary mucinous neoplasms (IPMNs), and a smaller proportion, 16.2%, had serious cystic neoplasms, while 15.1% had mucinous cystic neoplasms. The question is: which of these lesions need to be operated on and which can be followed by a ‘watch and wait’ policy?
The radiological classification of IPMNs divides them into two main types:
Main duct – which includes several types, with pancreatic IPMNs having the worst prognosis; 30–50% of lesions of this type are associated with cancer. This type of IPMN should not be managed with a watch and wait approach.
Branch duct – including gastric IPMNs, which have a good prognosis, meaning that a watch and wait approach may be better than surgery.
Clinical relevance of pancreatic cystic neoplasms: treatment or watchful waiting?
Beat Gloor (Bern, Switzerland) considered how to manage pancreatic cystic neoplasms, comparing surgery to watchful waiting. Historically, cystic lesions or IPMNs were classified according to their size, and decisions were taken on this basis, with recommendations published in 2010 (Pancreatology 2006, 6:17e32). A second major consensus – the Sendai Guidelines, which were developed by a Japanese consortium (Pancreatology 2012, 12:183–197) – focused on high-risk features: a solid component, ductal dilatation and mural nodule, to help clinicians decide whether an IPMN lesion is high risk and should be operated on.
There is no debate about IPMNs that have a bad prognosis – they should be operated. However, the situation is different for side-branch IPMNs, which have a good prognosis; here there is a debate about whether to watch and wait or operate. One of the key publications challenging this classification is a study by Stefan Fritz et al. of 512 consecutive operated patients with IPMNs at the European Pancreas Centre, led by Professor Büchler. The study included 148 patients with Sendai-negative branch duct type IPMNs, who should not have been operated on based on this classification. However, 26% of them were found to have high-grade dysplasia or invasive cancer.
If the group had not operated on these 148 apparently low-risk patients, they would not have discovered that 26% of them required surgery. A further 29% had main duct involvement, even though imaging had indicated they had side-branch IPMNs – and main duct IPMNs should undergo surgery (Ann Surg 2014, 260:848–55, discussion 855–6). This study of real-life clinical practice taking a more aggressive approach to surgery challenged the notion that the Sendai guidelines represent good practice.
The thoughtful but provocative report drew criticism from the pancreatic group at the Memorial Sloan Kettering Cancer Center (Ann Surg 2014, 259:e45). They have a much lower number of Sendai-negative IPMNs but they do have some, even though there should be none based on the guidelines. They reported quite notable postoperative mortality of 2%. They felt that operating on the large number of patients, as reported by Fritz et al., could not be justified, and advocated a watchful waiting policy in this situation.
Gloor recommended that, in general, mucinous neoplasms and main duct IPMNs should be operated. For IPMNs not in this category, discussion should focus on: where the lesion is located – for example, for lesions in the pancreatic tail, surgery would not mean whole pancreatic resection; the patient’s performance status; and the centre’s surgical expertise. I consider this recommendation quite pragmatic, and we can adapt this according to a centre’s practice and the number of patients undergoing resection.
Question:What do you think personally? If patients think they may have a pancreatic tumour, they usually want to have it removed. What do you say to these patients?
Answer: The paper from the Büchler group showing so many cases that, in the end, should have been operated, might suggest the guidelines are very defensive. But, on the other hand, I was surprised to see the high mortality rate. In my centre, where we operate on fewer cases, we would probably be more cautious in operating, weighing up whether the mortality justifies this, and recognising that the complication rates may potentially be higher in a smaller centre. Expert centres can probably deviate from guidelines and still have acceptable outcomes.
Question: How do you watch these patients if you don’t operate? Would you see them every three months? What’s your policy?
Answer: In our centre we decide on a case-by-case basis. Endoscopic ultrasound and MRI play an important role, but there is no clear recommendation on how frequently this should be done.
Improving outcomes: a case for neoadjuvant radiochemotherapy
Karin Haustermans (Leuven, Belgium) reviewed the role of neoadjuvant radiochemotherapy in pancreatic cancer. This is sometimes rather neglected, with oncologists often stressing the role of chemotherapy. In terms of clinical presentation of pancreatic cancer:
10–15% of patients are deemed operable
30–40% of pancreatic cancers are locally advanced, and can be classified as (i) those that are clearly inoperable, which are currently treated primarily with chemotherapy, and (ii) borderline cases, where neoadjuvant radio-chemotherapy can be discussed
a further 40% of cases are metastatic.
Focussing on borderline locally advanced pancreatic cancers, the advantages of neoadjuvant treatment are that it avoids unnecessary surgery in patients with poor prognosis who would progress anyway (25%); it treats micrometastatic disease; and can increase R0 resection, particularly in the retroperitoneal margin, which can sometimes be difficult to tackle. Radiochemotherapy is primarily useful in reducing unnecessary surgery and increasing R0 resection.
An extensive review (PLoS Medicine 2010, doi:10.1371/journal.pmed.1000267) showed the impact of neoadjuvant radiochemotherapy on borderline tumours includes:
significant downstaging and downsizing
a decrease in positive margins from 26% to 12%
improved tolerance of treatment – there are fewer complications, notably fewer fistulas, if radio-chemotherapy is given before surgery rather than afterwards, and
50% of cases become resectable.
I was surprised by these data. The halving in positive margins and 50% of cases becoming resectable make this approach look very promising. However, there is a problem in defining positive margins. I do not know which classification of positive margins was used in this review, but there are different classifications, with the Büchler group’s criteria finding almost 75% of all operated pancreatic cancers have positive margins.
Two prospective phase II studies have investigated pre-operative radio-chemotherapy in borderline resectable pancreatic cancer. One of these, from the MD Anderson Cancer Center, included 132 consecutive patients with tumours of the pancreatic head (adenocarcinoma) treated with preoperative chemoradiation followed by pancreaticoduodenectomy between 1990 and 1999 (Ann Surg Oncol 2001, 8:123–32).
Patients with no tumour progression before planned surgery went ahead to pancreaticoduodenectomy. Results showed the overall median survival from the time of tissue diagnosis was 21 months (95%CI 19–26 months). Survival was significantly longer for women (P=0.04) and for patients with no evidence of lymph node metastasis (P=0.03). There was no impact of age, dose of preoperative radiation therapy, delivery of intraoperative radiotherapy, tumour grade, tumour size, retro-peritoneal margin status or the histologic grade of the chemoradiation treatment effect.
Molecular differences between intra- and extrahepatic cholangiocarcinoma
Jean-Charles Nault (Paris, France) gave an interesting presentation on molecular differences between intra- and extrahepatic cholangiocarcinomas. Cholangiocarcinomas have a very heterogeneous pathology (see figure), with intrahepatic tumours and extrahepatic (hilar and distal) cholangiocarcinomas.
Cholangiocarcinoma: a heterogeneous cancer
In addition, gallbladder cancers can occur in the cystic duct or the ampulla. Location can influence prognosis, so it is important to be clear on this in reported outcomes of studies. Cholangiocarcinomas are intrahepatic in 10–20% of cases, and extrahepatic in 80–90%, with 50–60% of these being hilar and the remainder distal type of gallbladder carcinoma.
Risk factors for cholangiocarcinoma unrelated to tumour location are liver flukes, primarily in Thailand and China, and autoimmune disease such as sclerosing cholangitis, but sporadic cases can also occur. Parti-cular risk factors for intrahepatic cholangiocarcinoma are hepatitis B and C, diabetes and alcohol.
The link with hepatitis B and C underlines the need for rigorous diagnostic workup, because it is difficult to differentiate cholangiocarcinoma related to hepatitis C from an hepatocellular carcinoma, but it may have repercussions for outcome and choice of treatment.
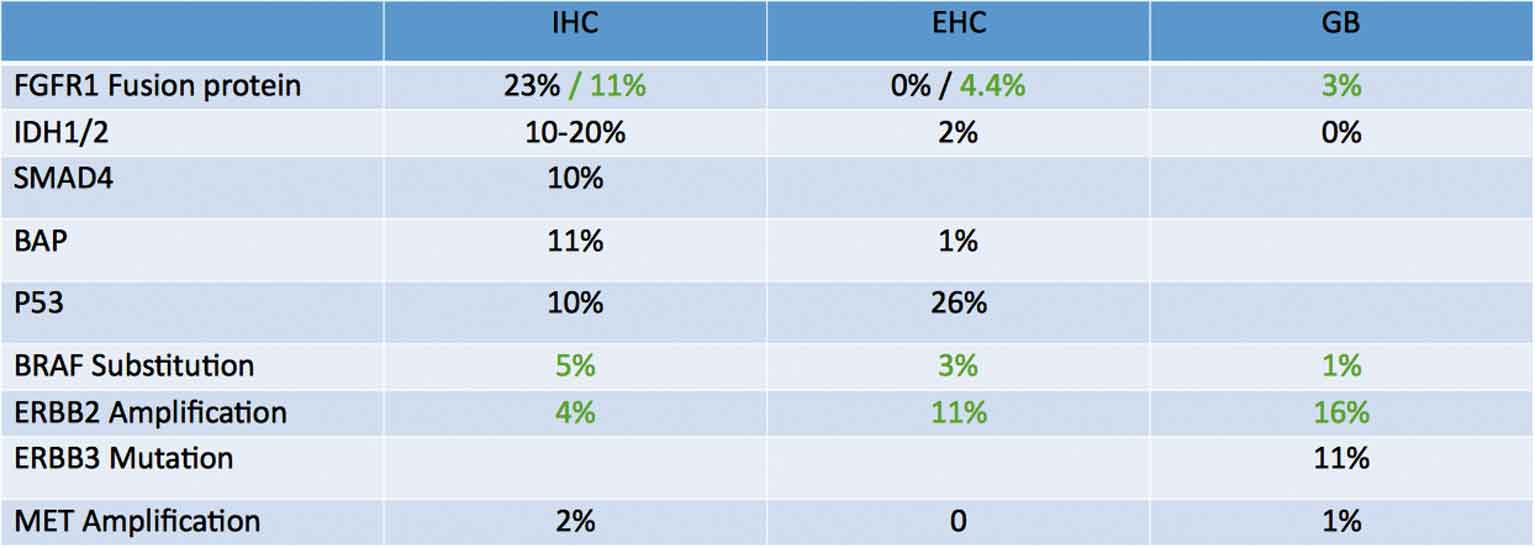
I have combined the information from two presentations at the St Gallen conference, one by Jean-Charles Nault and the other one by John Bridgewater (London, UK) (see table).
Genetic landscape of cholangiocarcinoma
Source: Adapted from JC Nault and PJ Ross, ASCO 2015; green figures are from John Bridgewater’s presentation, which was based on the ASCO presentation by PJ Ross (click to enlarge)
It is interesting to look at some of these genetic targets and their distribution in terms of where a cholangiocarcinoma is located:
FGFR1 fusion protein is a type of fibroblast growth factor, which can be targeted by TKIs, and occurs at a frequency of 23% in intrahepatic cholangiocarcinoma (IHC), but is much less frequent in extrahepatic and gallbladder cholangiocarcinoma.
IDH1 mutations are also frequent in IHCs, but to a lesser degree in extrahepatic and gallbladder cholangiocarcinoma.
HER2 amplification occurs in up to 16% of gallbladder cholangiocarcinomas, although other studies report a lower figure of 7–10%. The HER2 rate in gastric cancer is about 10% in unselected patients, so the rate of 16% in gallbladder cancer seems to be quite promising. ERB3 was reported only by Nault, with a rate of 11% mutated in gallbladder cancer. It seems that ERB2/3 signalling is quite relevant in gallbladder cancer, and may be amenable to different treatment strategies. In contrast, MET amplification does not seem to be very relevant.
Potential therapeutic targets and their respective drugs are:
FGFR2: ponatinib
IDH1/2: the inhibitor AGI-5198 could be promising
BRCA1/2: a PARP inhibitor such as olaparib in combination with platinum
PI3CA: everolimus
BRAF: vemurafenib.
It would be interesting to screen for these mutations in a trial. However, before doing this we should see whether there is any indication from clinical data that these mutations may be influenced by ethnicity or gender. We may then be able to enrich patient groups so that every patient does not have to be screened for everything.
Question:At a rate of 16% in gallbladder cancers, is it justified to assess HER2 amplification in every gallbladder cholangiocarcinoma patient? Also, should we look for other mutations? Should we do a panel? It’s a rare cancer and we don’t have good options.
Answer: There is one aspect that is not highlighted here, which is whether the observations summarised in the genetic mutations table are linked to ethnic background. Given that biliary cancers have very different prevalence and origins in people from Europe, Asia or South America, the first step I think we need to take is to see how these reported frequencies correlate with where patients come from and the origin of their biliary tract cancers. I have looked at HER2 amplification in Swiss patients and, particularly in gallbladder cancer, I found that HER2 was amplified in two or three Swiss-Italian patients and treatment was extremely efficacious. In Qatar we have a Bangladeshi female patient whose gallbladder cancer is focally HER2/3 positive. The problem is that we don’t have a pathway for standard pathologists giving a reason for testing for HER2/3, so it is still an individual decision. If a pathologist is willing to perform this testing, then I think it is worthwhile, because we don’t have other treatment options in second line. However, it is difficult to argue for this if someone asks for the data.
Question:Intra- and extrahepatic cholangiocarcinomas are quite different genetically. Do you design first-line chemotherapy using this information? Do you use standard cisplatin/gemcitabine or do use treatment depending on genetic data?
Answer: Personally, I use gemcitabine/cisplatin chemotherapy. I know some of my colleagues prefer gem-citabine/oxaliplatin (GEMOX), probably for historical reasons. The trial by Valle (NEJM 2010; 362:1273–81) gave only six cycles, but I have the impression that there is a subgroup of patients who respond very well to chemotherapy and we can go beyond six cycles in these patients. However, patients may have a very benign evolution even though their cancer is metastatic, so they may not need any chemotherapy and can be managed clinically. It is difficult to know, so one would always see how chemotherapy is tolerated and continue as long as possible.
Patterns of recurrence after surgery for extrahepatic cholangiocellular carcinoma
The pattern of recurrence after surgery is an important consideration and was reviewed by Stefan Staettner (Innsbruck, Austria). A Korean study looking at patterns of initial disease recurrence after resection of biliary tract cancer included 231 patients with hepatobiliary cancer, intrahepatic cholangiocarcinoma (IHC) or extra-hepatic cholangiocarcinoma (EHC) who underwent curative resection (Oncology 2012, 83:83–90). Results showed recurrence in gallbladder cancer and IHC occurred after a significantly shorter time than for EHC, and location had an important impact on outcome. In the case of local diseases, recurrence occurred after 6.3 months and 6.7 months for gallbladder cancer and IHC, respectively, com-pared to 13.1 months for EHC. For distal disease, recurrence occurred after 5.8/6.5 months (gallbladder/IHC) versus 14.1 months (EHC). Any trial that is planned should take this into consideration.
Staettner commented that multi-variate analysis showed that several factors, including distant recurrence tumour marker, lymph node status and lymphatic invasion, are correlated with poor prognosis but, surprisingly, a positive margin (R1) was not a poor prognostic factor. However, hilar and distal EHCs were combined in the Jung study, and the overall survival for these patients was 48 months, which seems an incredibly long time.
A second study covered 479 patients with biliary tract cancers from two tertiary centres in Italy (Bologna and Verona) between 1980 and 2011 (Eur J Surg Oncol 2015, 41:1162–9).
This included 172 cases of IHC (36%); 243 cases of perihilar EHC (51%); and 64 cases of distal EHC (13%). Multivariate analysis showed that only microvascular invasion was signifi-cantly related to long-term outcomes. Staettner commented that the overall survival was only 23 months (50% less than the Korean study) and, although there was a large number of patients, the study covered a long period of time and adjuvant therapy was not reported.
In summary, the survival rate after curative resection was 20–40%, the rate of positive resection margins (R1) was high, but this did not seem to have an impact on overall survival. Staettner noted that recurrence occurs mainly within 24 months, and there are subgroups of patients who have primarily local recurrence and others who have upfront distant recurrence, and these may need to be tackled differently. Surgical morbidity is an issue that has not been studied extensively so far.
Improved outcome in extrahepatic cholangiocarcinoma with radiation therapy
Gian Carlo Mattiucci (Rome, Italy) reviewed the impact of radiation therapy, which is a topic that attracts a lot of discussion in our tumour board. The challenges are that almost all data are retrospective, patient groups are heterogeneous, and conclusions are based on small numbers. The key publication is a comprehensive systematic review of the literature, including one randomised trial, two SEER registry analyses and 17 institutional reviews (JCO 30:1934–40). The sobering news was that there was no improvement with adjuvant radiochemotherapy for the study pop-ulation overall, or for patient subgroups, although there was an impression of improved outcomes for margin-positive and node-positive disease. However, the benefit was seen only if the two SEER studies were excluded, with an advantage with chemotherapy for node-positive disease and with radiochemotherapy for positive margins.
Overall, there are probably no real data supporting the routine use of adjuvant chemotherapy, and specific discussions are needed for patients where surgery is insufficient or should not have been done. Adjuvant chemotherapy should not be used to cover up insufficient surgery.




 This grandround was first presented by Jonas Feilchenfeldt, from the National Center for Cancer Care and Research (NCCCR), Doha, Qatar, as a live webcast for the European School of Oncology. It is edited by Susan Mayor. The webcast of this and other e-sessions can be accessed at e-eso.net.
This grandround was first presented by Jonas Feilchenfeldt, from the National Center for Cancer Care and Research (NCCCR), Doha, Qatar, as a live webcast for the European School of Oncology. It is edited by Susan Mayor. The webcast of this and other e-sessions can be accessed at e-eso.net.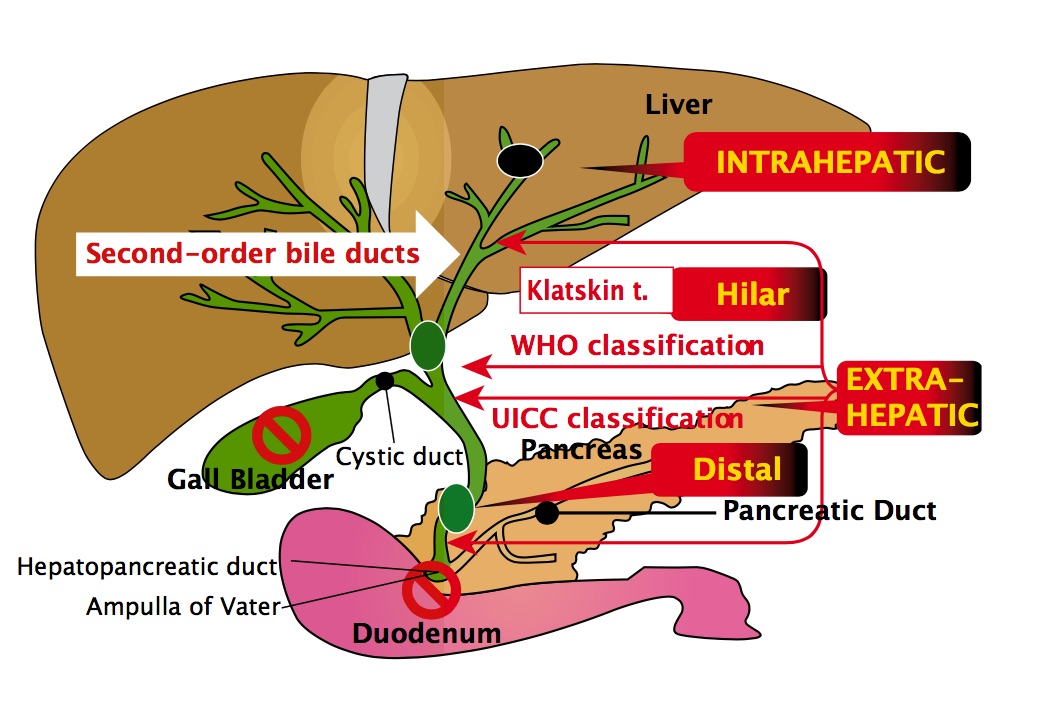


Leave a Reply