Antonella Cardone, Director of the European Cancer Patient Coalition and Board Member of All.Can Brussels, opened the session with a brief recap on All.Can and its initiatives.
All.Can is an international multi-stakeholder platform, a thought-leader in cancer care in Europe and beyond. Since 2017 it has produced several publications, starting with “Towards a Sustainable Cancer Care”, and has conducted extensive surveys on patient insights over the years. In 2020 it began to work on the “efficiency hub”, an ongoing project that collects best practices in cancer care. On 27 May 2021, All.Can International launched its latest policy report, “Harnessing data for better cancer care”, which assesses the essential role of data in cancer care to improve outcomes for all people with cancer. The efficiency hub aims to collect and showcase real-world examples of initiatives shown to improve efficiency in cancer care, in order to create a learning community around best practice examples. In Part 1 of this webinar, we heard about three initiatives, and another three were presented today.
Example 1: A MASCC Designated Centre of Excellence in Supportive Care in Cancer
Andrea Antonuzzo, Medical Oncology – Pisa University Hospital, Head of the Supportive Care Unit
In the oncology department of Pisa University Hospital, a supportive care service (SCS) for cancer patients was created in 2012 and last year it received certification from the Multinational Association of Supportive Care in Cancer (MASCC) as a centre of excellence. To borrow the definition given by Jean Klastersky, supportive cancer care is like “an umbrella which would protect the cancer patients from the earliest stages of the disease until its end, in order to maintain a ‘quality of life’ as desirable as possible.” At Pisa University Hospital, the oncology department is divided in an outpatient clinic for day-hospital treatment and a small in-patient unit. The SCS is conveniently located on the second floor of the building – a real model of simultaneous care for cancer patients. It is open daily from 8am to 2pm and provides several services: diagnosis and treatment of drug toxicities; cancer symptoms management; diagnosis and treatment of comorbidity and cancer complications; administration of bisphosphonate and hemoderivatives (mainly red blood cell transfusion), and more. At the beginning of therapy, all the patients are given an informative brochure, so they know what services are available and where to go.

The SCS works together with the oncologist, the transfusion centre, and other specialists, such as dermatologist, pain specialist, nutritionist, but also psychologist and chaplain, because sometimes, beside clinical and physical help, we also need psychological and spiritual support. Every year the centre manages more than 1,000 unplanned visits, and can organise all the therapies that the patient requires on the same day without an appointment. Also, at the beginning of anticancer treatment patients receive a dedicated mobile phone call number, so they know that they can interact with the centre also by phone.
Changing the ‘’route’’ of cancer patients
This kind of support is appreciated by patients and their families because they know from the start that they can liaise directly with the SCS, without having to go to the emergency room or to the general practitioner. A short paper by Dr. Antonuzzo and his team, published in Supportive Care in Cancer in 2017, shows that the introduction of the dedicated centre in their oncology department in 2012-2013 caused a substantial decrease in the number of unplanned hospitalizations of on-treatment cancer patients compared to the previous year. This is a move in the right direction also financially because the hospital and the entire healthcare system may obtain a reduction in cost for cancer patient management. The SCS has started to manage blood supported care services as well, with same day red blood product transfusion. This also helps reduce costs, as the same service provided in the emergency room would be much more expensive.

A look into the future: education and implementation
It is important to run educational programmes for young post graduate MDs, with monthly hospital meetings on supportive care issues and interactive discussion and reporting of clinical cases.
In the future the SCS’s activities will expanded, with a medical oncologist close to the emergency room, because this way, the team can manage a direct consultation service for acute medicine in the same hospital. Beside the medical oncologist, probably Dr. Antonuzzo himself, a pain specialist and another medical oncologist will join the team for palliative care. Recently the hospital has approved this plan. So, with these two services, the supportive care service and the palliative care consulting team, a global supportive care can be offered.
The second presentation was by Elizabeth Hanson, Board member and prior President of Eurocarers, Professor of Health Care Sciences, Linnaeus University, Sweden, Research Director, Swedish Family Care Competence Centre.
Example 2: Examples of best practices from Eurocarers
Eurocarers is the European association working to support informal carers across Europe. It comprises relevant research centres and university departments, carers’ organizations, and individual members with an interest in carers. But who are informal carers and how many are there? They are primarily family members, but they can also be friends, extended relatives, work colleagues, neighbours, who provide usually unpaid care on a regular basis to someone with a chronic illness, disability, or other long-lasting health or care need, such as a person living with cancer, outside of a professional or formal framework. They are predominantly women, and they make up as much as 10-20% of the total EU population. The estimated value of informal care in Europe is between €320 and 368 billion. Without the substantial input of informal carers, our healthcare systems would collapse overnight, so it is crucial that they receive the support they need. The impact of caring varies, some caregivers find it satisfying and meaningful, whilst others find it stressful and burdensome. Women to a greater extent than men experience caring as physically and mentally demanding. Higher intensity caring and longer hours often carry a ‘triple penalty’: it can affect the carer’s own health and wellbeing; work life/care balance; social and financial situation. A recent survey carried out by Eurocarers shows that the COVID-19 pandemic exacerbated the situation for many carers across Europe, as they had to deal with more intense responsibilities and more hours of work (+17% weekly hours). There was also an increase of more than 10% in the number of carers. Furthermore, the Global Care Well-Being Index 2021 identifies cancer carers as a risk group: 71% of cancer carers say the COVID-19 pandemic has made caregiving harder.
How best to support informal carers
There are four key-elements to consider:
- Recognition: we need to reach out, recognize and identify carers of people living with cancer, as soon as possible and, wherever possible, carry out an assessment of their needs and preferences, as well as those of the cancer patient.
- Information: carers request a lot of information, e.g., cancer patient’s diagnosis, prognosis, treatment regime, symptom management, financial benefits available, local sources of support.
- Education and skills training: particularly those carers that have never had any prior experience of caring often require education and skills training, individual and/or in group format, in order to care effectively and efficiently without harming themselves or the person they are caring for.
- Support: carers need emotional support to reduce stress, such as support groups, individual counselling and supportive conversations; also, practical help with caring, and assistive devices; they often require financial support and, particularly for those high-intensity carers, respite care, i.e., access to regular breaks from caring. It is very important to highlight that there is no one-size-fits-all when it comes to support: it must be tailored to the needs and preferences of the individual carer and the phase of caring they are in.

The following good practice examples come from Eurocarers members in the respective countries concerned:
Improving the Cancer Journey (ICJ) in Scotland
Launched in Glasgow in 2014, Improving the Cancer Journey (ICJ) is an integrated care service which aims to improve the outcomes of people affected by cancer. Since its initiation ICJ has been set up in some local authority areas in Scotland, including the Edinburgh area (the Lothians) in 2021. Its approach centres around a Holistic Needs Assessment (NHA), both for the cancer patient and their carer. A dedicated Link Worker (LW) coordinates the care for the patient and their carer and develops a care plan together with the client that can then be shared with other healthcare staff. The LW provides a “listening ear” and further support. The care plan is reviewed at 12 weeks. The LW knows the local communities well and engages with a wide range of services and resources. From the data that is being collected on an ongoing basis by the Napier University in Edinburgh, about 1 in 10 people who have accessed the Lothians service has been a carer. Their priorities have been the following: reduced stress and improved wellbeing, financial advice, reduced social isolation, and help to navigate the health and social-care system. This is a great example of an integrated care service, and it shows the importance of a link-worker and a dedicated care plan.
Mantelzorg Balans website in the Netherlands
The second example comes from the Netherlands. Mantelzorg Balans is a newly established website (https://balans.mantelzorg.nl/) co-created by informal carers of people with cancer and healthcare professionals. It was launched early in 2021 as “many informal carers care with love for a relative who is terminally ill, yet often find it difficult and stressful”. The website stimulates carers to reflect on their own preferences and helps them make choices in line with their own limits, and to achieve balance in their lives. It has also a range of exercises and targeted information for informal carers such as “things to arrange” for terminally ill patients, finances, sources of support for carers, and so on. It even has a dedicated private page only accessible by the carers where they can document memories. The initiative is currently being evaluated by the University Medical Center in Groningen. The Netherlands offer much innovative online support, for instance a dedicated website for children of cancer patients.
Compassionate Care Allowance: Sweden
Compassionate Care Allowance exists in many countries, with different levels of coverage and amount, but Sweden is a more generous example. Carers can apply to the Swedish Social Insurance Agency (SSIA) for an allowance that enables them to take paid leave from work to care for a family member/significant other who is seriously ill, irrespective of whether s/he is at home or in hospital. The application form is completed by the carer and requires a written physician’s opinion and consent from the sick person. The allowance can be paid out for a full day, or a percentage of the day, for a maximum of 100 days. It covers roughly 80% of the salary. If the time perspective is uncertain, the carer may take out some allowance days and then pause it for a while if the condition of the cancer patient stabilizes. The SSIA statistics highlight that the majority of those who access the allowance are female working carers. Financial support is something that carers often request, and the Swedish system is a pretty good model in this respect.
Family centred approach: Sant’Orsola Malpighi Polyclinic, Bologna, Italy
The oncology department of this Italian hospital has a holistic, multi-disciplinary approach, focussing on both the cancer patient and his/her family. They cover the entire cancer trajectory and different pathways are offered, as appropriate. There is psychological support already at the time of diagnosis and daily presence on the ward, with extra interventions in crisis situations. Individual interviews are carried out with children of patients and other family members on a weekly or fortnightly basis, and there are also group meetings. A comprehensive range of complementary therapies is on offer (weekly sessions run from October to June), with theatre workshops, music therapy, meditation, dance therapy, writing, drawing, and photography workshops. The department carries out awareness raising and education with vital stakeholders in the region: local meetings with schools, associations, primary health care physicians. It also runs training courses for informal carers, so healthcare professionals know more about them and how to best support them. During the COVID-19 pandemic, online deliveries were also activated. Another positive aspect of this system is that they carry out routine evaluation in the form of user satisfaction questionnaires, and research in the form of graduate theses. The results of this family centred holistic approach indicate a significant reduction in anxiety, depression, somatisation, and an increase in levels of physical well-being, security in relationships, cognitive restructuring skills, problem solving, acceptance of change and sense of personal competence, for participant cancer patients and family members.

Recognition, information, education, and support are key to supporting carers. Support must be tailored to the needs and preferences of the individual carer and the phase of caring they are experiencing. Financial support is often valued and requested by carers, yet in many countries economic benefits are not always prioritised by politicians or decision makers. Multi component, dyadic and whole-family approaches often have greater impact on people living with cancer and their carers than single component approaches. Supports that are integrated within the existing health and care systems are more likely to have greater effect on patient and carer outcomes, ensure a higher take-up of the service and be sustainable over time. More flexible hybrid approaches (mix of face-to-face and online) have been offered during the COVID-19 pandemic to support carers. Although, online approaches do raise issues of equal access, such as the risk of social exclusion of more vulnerable groups of carers because of lack of digital literacy skills, and/or access to information and communication technologies.
The last speaker was Alexander Roediger, Global Lead Oncology Policy, MSD International, Kriens, Switzerland, who presented some evidence research his team has conducted in the past few months to assess the efficiency of lung cancer patient journeys and what can be done to improve it.
Example 3: More Efficiency = Better Outcomes. Timely treatment in lung cancer
Treating patients early leads to better outcomes. If cancer is detected early enough, the five-year survival is much higher than if discovered at a later stage, when it has metastasized. Looking at lung cancer, we see that the five-year survival is 60% if diagnosed at the local stage. But if it is already at a distant stage, the chance is reduced to 6%. Unfortunately, most lung cancer cases are diagnosed at a late stage, so, compared to some other cancer types, like breast or melanoma, lung cancer patients have much worse outcomes. Comparing mortality rates of different cancers, lung cancer is among the ones in which progress has been made in terms of treatment, but in terms of outcomes it still rates very low. If patients are diagnosed, do they get treatment? MSD commissioned a study on drug treatment rate in advanced NSCLC (non-small cell lung cancer) in Europe, which was published in September in the ESMO’s Annals of Oncology. Treatment rate is the percentage of eligible patients who get access to treatment. No country has 100% treatment rates, there are always patients who never reach treatment. Rates differ greatly in different countries: in Belgium, Hungary, Norway, and Portugal, they are around 72-81%. In Bulgaria, Finland, Ireland, Netherlands, the percentage is 50%, meaning that only one out of two eligible patients gets treatment. Poland, Romania and the UK have registered the lowest rates (36-43%). Something is obviously not working: treatment is available, but not every patient gets access to it. Looking at the types of treatment, chemotherapy is of course the standard, but from 2016 immunotherapies have become available, also targeted therapy, but different countries have different uptakes of these innovations. Early diagnosis is very important, but so is access to treatment once the patient has been diagnosed. One of the reasons for the difference in treatment rates is the complexity of a patient’s journey. Patients can be lost if the system is not working properly.

Improving the lung cancer patient journey delivers better outcomes
A person may have symptoms or live in a country that has routine screening programmes. If the screening detects lung cancer, more screenings and tests are carried out, followed by diagnosis, treatment discussion and treatment. But patients can remain untreated for various reasons. It may be due to poor diagnosis, or even to treatment refusal: some patients do not accept the fact that they have lung cancer. Sometimes, because of innovation, treatments have become more complex. We are in the age of personalized medicine. So, very often a biomarker test is required. Patients are tested, and the result usually must be interpreted by someone else, the pathologist, before it goes back to the treating specialist. Some countries may not have enough pathologists, so tests are made, but it takes a long time for the results to reach the treating physician. There may also be strict eligibility criteria, so that certain innovations are less accessible in some countries than in others.
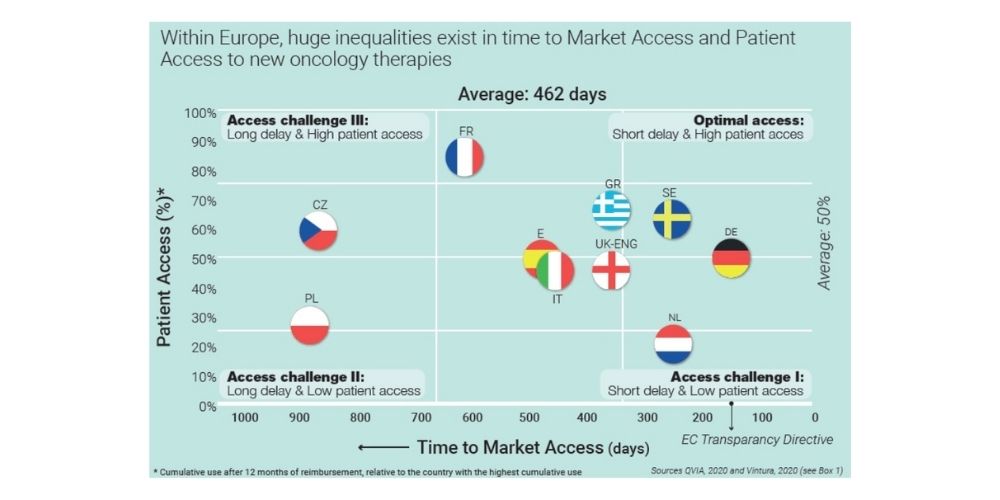
Another issue is that patients may receive outdated treatment options. A new medicine must be authorised for marketing by the European Medicines Agency (EMA) that assesses its efficacy, safety and quality. Then the European Commission makes the final decision. But how does a new medicine get into the system? It needs to be reimbursed. The payer or the government must decide whether it should be added to the reimbursement list so that the patient can access it via private or public health insurance. Time to market access varies dramatically from country to country, it is very fast, for example, in Germany, just over 100 days. The Netherlands and Sweden are second on average with between 200 and 300 days, but there are other countries such as Poland, or the Czech Republic, where it takes up to 900 days. So, there is a ninefold difference between the fastest and the slowest country. The other question is how many patients receive the treatment 12 months after reimbursement? France for instance is relatively slow in reimbursing, more than 600 days, but in terms of uptake, it does much better than Germany, with 8 out of 10 eligible patients vs 1 out of 2.

Learnings from lung cancer – treating cancer early improves cancer patients’ outcomes
The earlier the cancer is detected and the more localized it is, the higher the chances of a five-year survival. A timely diagnosis is critical and can be improved through symptom awareness (health literacy of both patients and healthcare professionals) and early detection mechanisms. But diagnosis which is not soon followed by treatment can be very harmful for patients. Timely access can be achieved through faster referral, testing infrastructure and human resources, and by reducing inequalities in the availability of treatments.
How to improve efficiency? A cross-country dashboard which includes treatment rates does not yet exist, but once you start to measure and identify the differences, you develop the urgency to address the issues. What is measured gets done: early diagnosis and treatment rates are important indicators to improve efficiency and cancer patients’ outcomes.
Next webinar










