A series of webinars called “Spotlights on Improving Efficiency in Cancer Care” and including 11 monthly meetings from December 2020 to October 2021 was just inaugured by SPCC. The First Webinar entitled “Improving Efficiency in Cancer Care” was held online on December 1st 2020. The webinars are international and will involve different continents (Latin America, Australia and Asia).
After the introduction by Chairman Pietro Presti, analysis of inefficiency and strategies for improving efficiency in cancer care were presented by Eduardo Pisani, Alex Filicevas, and Stefan Gjssels.
Eduardo Pisani is CEO of All.Can International, Brussels, Belgium.
From the pages of CancerWorld we talk about new treatments, prevention, health policy, medical societies and patient’s voices in oncology as well as affording several other broad topics. It is extremely important to us focus also on efficiency in care.
Information based on analysis made by The World Health Organization, the OECD, and other agencies is available, estimating that by removing ineffective interventions and any other wasteful interventions, there could be savings up to 20% in healthcare spending across Europe. One impact of inefficiency is due to the lack of treatment adherence: the non-respect of adherence is costing to Europe 125 billion euros.
But what is efficiency?
Existing definitions of efficiency are mostly driven by health economists and healthcare professionals, with outcomes often based on processes that are easily measurable within healthcare systems. Besides the financial savings, even more important is the fact that there could be a gain of approximately two years of life expectancy by being more efficient. This is what mostly matters to citizens and patients in particular. Patients have directly full sight of the impact of their condition and care experience on their physical, emotional and mental wellbeing. “Efficiency is not only synonym of cost containment.”
Inefficiencies in care coordination can lead to significant delays in several sides of care. Redesigning the entire process could decreases patient’s waiting time for screening and diagnosis, improves resource utilization, allows scheduling on patient visits, individualize patient care, eliminate unnecessary waste processes, reallocate health-care providers’ time, improve patient satisfaction.
Bullet points from Eduardo Pisani Presentation are reported here:
- Ineffective, unnecessary or even harmful healthcare interventions lead to poor outcomes or outcomes not in line with cancer patients’ needs
- For cancer patients, healthcare inefficiencies can lead to a reduction in their quality of life, financial and time losses, as well as to inequities between different groups in society
- Healthcare inefficiencies weaken health systems, services and processes, and lead to significant financial loss and missed opportunities for freeing up human and financial resources to allow continuous improvement within the healthcare system
- Inefficiencies can demoralise and frustrate care providers, who feel unable to give the quality of care to their patients, which they deem appropriate and optimal
- Inefficient healthcare systems are less resilient, adaptive and innovative. In the field of oncology, the increasing disease burden and complexity of cancer management require high levels of resilience, rapid adaptation of practices and innovation
Alex Filicevas is an Executive Director of World Bladder Cancer Patient Coalition and President of the Board of All.Can International. His talk focused on Patient’s needs. All.Can has designed a patient survey to the purpose of gaining a better understanding of where patients consider their care is not focused on what matters to them.
Patients where asked whether they had encountered inefficiency across the entire continuum of cancer care, including diagnosis, treatment and care, ongoing support and the broader impact of cancer on their lives. The survey questionnaire revealed major inefficiencies.
Nearly 4,000 participants who were patients and caregivers participated to the survey from more than 10 countries, representing the largest international survey of its kind. All.Can states than when we talk about ensuring value in the way we deliver care, we often don’t define this specifically from the patient and caregiver perspective.
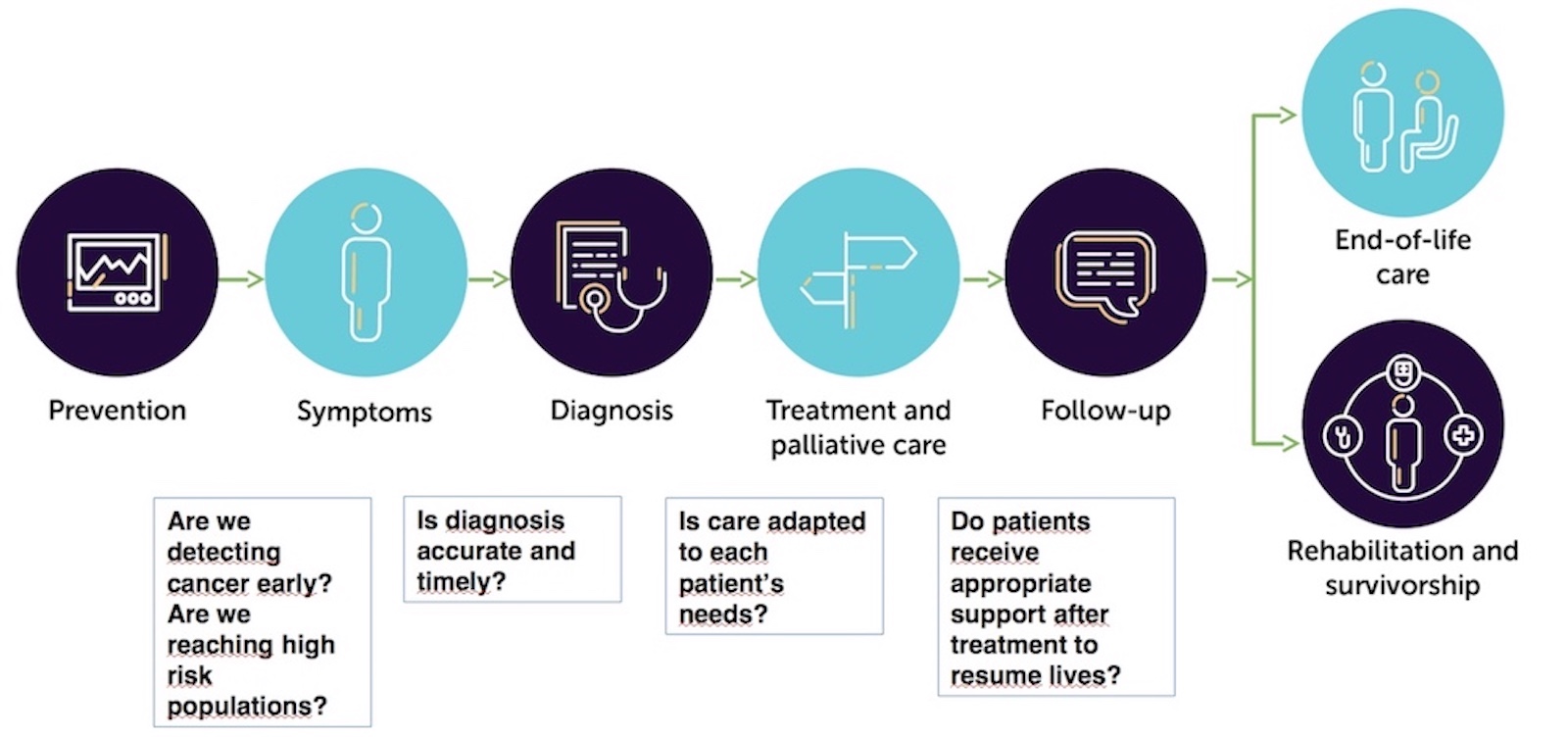
The results were published https://www.all-can.org/reports/all-can-patient-survey/ providing very relevant information. Based on this survey I am outlining the various “check-points” where efficiency is debated.
Prevention Symptoms Diagnosis Treatment and Palliative Care Follow up Rehabilitation and survivorship End-of life care
Key findings of the survey are summarized below:
- About: Swift, accurate and appropriately delivered diagnosis – 31% of respondents whose cancer was detected outside of a screening programme said that their cancer was diagnosed as something different – either initially or multiple times – 12% of respondents whose cancer was detected outside of a screening programme waited for more than six months to be diagnosed with cancer
- About: Information, support and shared decision‐making – 41% of respondents did not feel involved enough in deciding which treatment options were best for them – 25% were not given enough information (in a way they could understand) about their cancer care and treatment – 31% did not receive enough support to deal with ongoing symptoms and side effects – including beyond the active phase of their treatment – 30% did not receive enough information (in a way they could understand) about the signs and symptoms indicating that their cancer might be returning or getting worse – 23% were not given information about patient groups, charities and other organisations that might be able to support them
- About integrated multidisciplinary care – 59% of respondents reported that they needed some form of psychological support during/after their cancer care but, of those, 31% said that it was not available
- About the financial impact of cancer – 68% paid for some part of their cancer care: 55% for private health insurance, 6% for care and treatment not covered by insurance, and 4% to avoid delays – 44% reported travel costs, 31% reported loss of employment, 10% reported loss of insurance and 9% reported childcare costs* (these data were relative to US)
I like, as a scientist-journalist, to underline a particular point made in the webinar: the disconnection between the language used by the doctors and actually what the patients could understand. Patients often did not know where to begin or what to ask, because their experience of cancer was new to them. And so, there are also comments, in the survey, that the information provided is not always tailored to the patient’s individual experience, or for example, the stage of their treatment. Information needs, of course, to vary from one patient to another and is influenced by many factors.
One should ask whether patients receive appropriate support once they get back to normal life.
As an example of a major impacting cancer type, delays in the diagnosis and treatment of colon adenocarcinoma are distressing to patients and clinicians. The time interval between the index colonoscopy and subsequent operative resection is a quality metric in many health systems. Potential delays in meeting the ultimate decision-maker (i.e., the surgeon) as well as the wait time for surgical resection represent significant psychological challenges for most patients.
Stefan Gijssels is Executive Director of Digestive Cancers Europe and EuropaColon. Stefan is a colon cancer survivor and he is dedicated to helping other people avoid getting cancer, as well as helping patients to get access to the best possible treatment. Stefan also acts as a health policy consultant, publicist and public speaker.
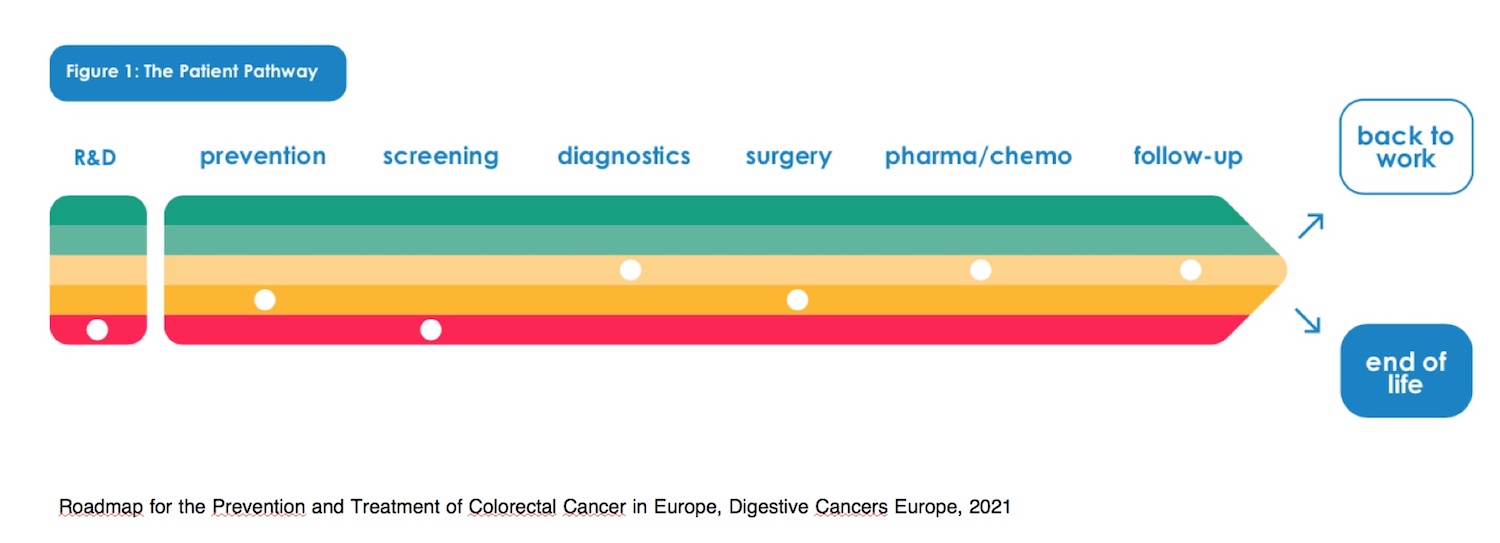
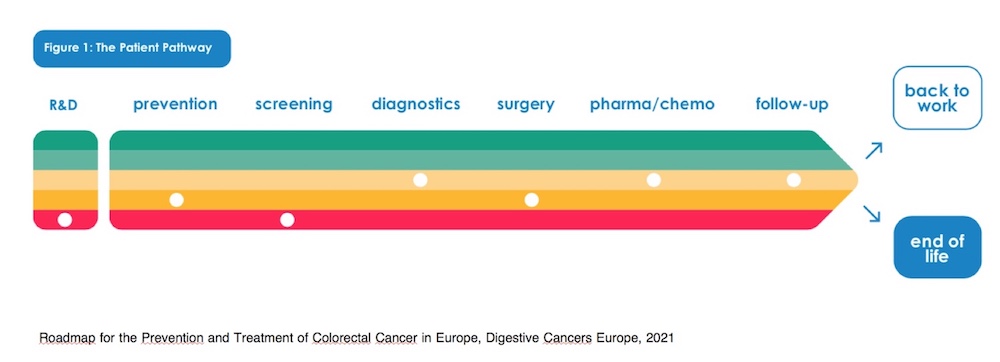
The associations are representative of all digestive cancer patients in Europe, with 32 member-organizations and they have defined their own value statement. So, the primary value is to work for patients, care-givers and the patient community in general: the collective group of patients. But at the same time, they aim to generate value for hospitals, for research industry, policy makers and the broader cancer community. They work on the patient journey, or the patient pathways, giving color-coding i.e red is not very good and green is very good, and white dots give the average in Europe as compared to the point where we should be.
Can Society afford not to be efficient?
Focussing on colorectal cancer, a disease that he personally knows well, Stefan Gijssels illustrate the following. These are the 4 stages of the disease. So, the 4 colours (see Fig) mean progression: the light green is stage 1; the red is stage 4. On average in Europe, the cost of treatment of somebody with a diagnosis in stage 1 is around 4,000 euros and on average 40,000 euros in stage 4. In his case for instance, the expenditure was 70,000 euros for metastatic colorectal cancer. The later we wait the more expensive the treatment becomes. But then if we look at the actual survival, (and this is not different from any other type of cancer), there is 90% survival in stage 1; and around 8 to 10% chance of survival five years after treatment in stage 4. This is an argument to say the system would be extremely sustainable and efficient, if on “puts the money” on the right place where it really matters to patients (Nicole Kloos, et al., Can J Surg., 2019) .
The Manifesto of Colorectal Cancer in Europe states:
- Every citizen between 50 and 74 years old should get screened with the latest type of test
- All citizens should be aware of their family history of colorectal cancer to be tested in a timely manner.
- All General Practitioners should be aware of the family history in colorectal cancer of their patients and if present, to have them tested in time
- Only Comprehensive Cancer Networks meeting the Essential Requirements of Quality Cancer Care in Colorectal Cancer should be allowed to treat colorectal cancer patients
- All citizens who are diagnosed with colorectal cancer should be directed to a dedicated colorectal cancer patient organisation
- All colorectal cancer patients should have access to their Electronic Health Record
- All colorectal cancer patients are entitled to the ten rights in the European Code of Cancer Practice .
One of my wishes towards efficiency in the Compehensive Centers is the implementation of molecular tumour boards even virtual (VMTB). A VMTB would systematically allow clinician to combine expert-curated data and structured data from clinical charts along with molecular testing data to develop consensus on treatments, especially those that require off-label and clinical trial considerations. (Michael J Pishvaian et al, JAMIA Open, 2019), which should improve efficiency in the hospital care. However, this is only one point in the entire cancer care pathway (see figures).
I conclude with Pietro Presti’s statement:
The main aim of the project on “Spotlights on Improving Efficiency in Cancer Care” of SPCC is to scale up and implement proven concept for reducing inefficiency in cancer care, supporting a patient-centric vision and the sustainability of a healthcare system while improving outcomes. The point is to design and develop a new international educational program in oncology on the theme of efficiency in cancer care that can embrace all relevant stakeholders.
The next webinar, Spotlights on improving efficiency in cancer care – Moving towards efficiency: Examples, will be held on January 13 at 18:00 CET









