The risk of dying from cancer is highest for men and women living in areas with greater poverty. A study into small-area variations in cancer mortality statistics between different English health districts, published in Lancet Oncology, 11 December, found that the risk of dying from cancer was more than 70% higher in the poorest areas in England than the wealthiest.
“Although our study brings the good news that the overall risk of dying from cancer has decreased across all English districts in the last 20 years, it also highlights the astounding inequality in cancer deaths in different districts around England,“ says Majid Ezzati, the senior author, from Imperial College London.
Cancer mortality in industrialised countries has declined more slowly than other major causes of death, leading to the proportion of deaths from cancers increasing over the past two decades. Small-area data, analysing information according to different health districts, offers the possibility to pinpoint exactly where primary prevention strategies and healthcare planning need to be enhanced to improve survival. “Small-area data on cancer mortality can… help assess how cancers contribute towards inequalities in all-cause mortality and life expectancy,” write the authors, adding that such data also offers the possibility to track progress following the introduction of interventions.
For the study, investigators analysed data from the English Office for National Statistics on deaths, between 2002 and 2019, from the 10 cancers responsible for the greatest death toll. For men, the cancers recorded were lung, prostate, colorectal, oesophageal, pancreatic, stomach, lymphoma and multiple myeloma, bladder, leukaemia, and liver. For women, the cancers recorded were lung, breast, colorectal, pancreatic, ovarian, lymphoma and multiple myeloma, oesophageal, corpus uteri, and stomach.
The team used the postcode of residence at registration of death to assign each death to a local authority health district, of which England had 314 in 2002. Then they used the proportion of the district population claiming income-related benefits (due to being out of work or having low earnings) to explore relationships between the risk of dying from cancer and poverty. Using a ‘Bayesian hierarchical model’, which allows exploration of patterns of mortality over age, districts, and time, the team obtained yearly estimates of the probability of dying from cancer between birth and 80 years of age. For the first time, write the authors, the methodology, allowed cancer mortality to be estimated for ‘small geographies’.
Results show that 2,453,173 deaths from cancer were recorded in England between 2002 and 2019, of which 1,533,703 (62.5%) occurred before the age of 80, with 697,953 (45.5%) being in women and 835,750 (54.5%) in men.
- Nationally, the risk of dying from cancer before 80 years of age declined for both sexes between 2002 and 2019, from one in six to one in eight for women, and from one in five to one in six for men.
- The Spearman rank correlation between probability of dying from a cancer and district poverty was 0.74 (95%CrI 0.72–0.76) for women and 0.79 (95%Crl 0.78–0.81) for men (CrI stands for ‘credible interval’).
- The strength of the correlation was due in part to strong correlations between district poverty and the probability of dying from lung cancer (Spearman rank correlation 0.76 for women and 0.85 for men), from stomach cancer (Spearman rank correlation 0.58 for women and 0.64 for men,) and from liver cancer (Spearman rank correlation 0.57 for men).
- Probabilities of dying from breast and colorectal cancer in women, prostate cancer in men, and pancreatic cancer, lymphoma and multiple myeloma, and leukaemia in both sexes showed little association with poverty.
- Some regions showed a larger decline than others. For women, the greatest district-level reduction in the risk of dying from a cancer was nearly five times that of the smallest (30.1% decline in Camden, compared to a 6.6% decline in Tendring). For men, the largest decrease was triple that of the smallest (36.7% in Tower Hamlets compared to 12.8% in Blackpool). Overall, districts in London (where Camden and Tower Hamlets are both located) achieved the largest decline.
- Variation in the probability of dying among women was largest for lung cancer, being 3.7 times higher in the district with the highest probability than in the district with the lowest probability. In men, the variation was greatest for stomach cancer, being 3.2 times higher in the district with the highest probability than in the one with the lowest probability.
“Our results on heterogeneous trends in mortality, particularly for cancers with modifiable risk factors and potential for screening for precancerous lesions, indicate that reducing these mortality inequalities will require factors affecting both incidence and survival to be addressed at the local level,” conclude the authors.
Commenting on the findings that lower mortality from specific cancers was observed in poorer districts in London than comparably poor areas elsewhere in England, the authors suggest the explanation could be due to differences in the quality of available healthcare. “Either because advanced treatments such as immunotherapies are more readily available, or because patients can travel to a specialist hospital rather than their local hospital because there is a higher density of hospitals.”
Some of the largest inequalities, add the authors, were observed for cancers strongly associated with behavioural and environmental risk factors, and those where screening for precancerous lesions was available. Access to diagnostic services was considered key to reducing the inequalities highlighted in the study, with people who are more deprived being less able to engage in cancer screening. “To change this, there needs to be investment into new ways to reach underserved groups, such as screening ‘pop-ups’ in local areas like supermarkets and working with community organisations and faith groups,” says Amanda Cross, one of the authors from Imperial College London.
Due to funding cuts, many English health authorities have reduced their budgets for smoking cessation. “Our data shows we cannot afford to lose these public health programmes and are in urgent need of the reintroduction and strengthening of national and local policies which combat smoking and alcohol,” says Theo Rashid, the first author of the study.
The data, the authors caution, only goes to 2019, underlying the need for further research to explore what happened to the risk of dying from cancer during the Covid-19 pandemic.
In a linked comment, Karri Seppä and Janne Pitkäniemi, from the Finnish Cancer Registry, write, “Cancer incidence is affected by factors that relate to the aetiology and diagnostics of the cancer, whereas population-based cancer survival data provides information on the differences in overall effectiveness of health-care systems during the entire patient pathway from health-seeking behaviour and availability of health services to diagnostics and treatment.”
High-resolution population-based cancer statistics, they add, are important to gain a more comprehensive picture of geographical variations in cancer burden. “These statistics might identify differences that are important for the prevention of new cancers and the improvements in early detection and cancer survival,” they write.
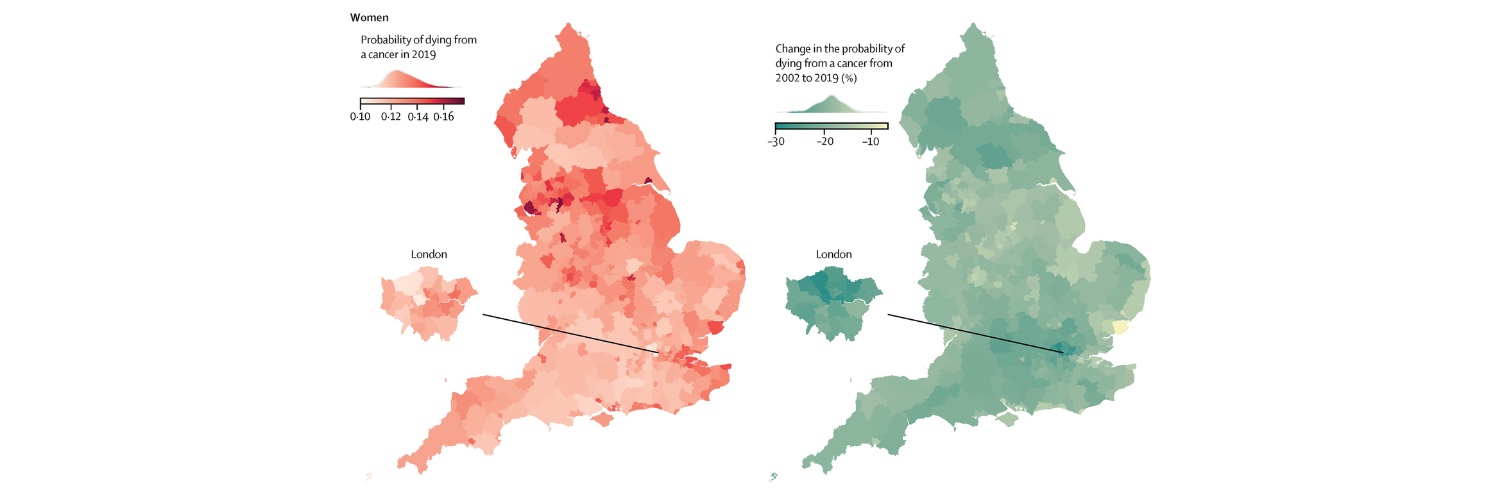
The opening illustration comes from Figure 2 in Rashid T, Bennett JF, Muller DC, et al. (2023) Mortality from leading cancers in districts of England from 2002 to 2019: a population-based spatiotemporal study. The Lancet Oncology. DOI:https://doi.org/10.1016/S1470-2045(23)00530-2. It is published here under a Creative Commons CC-BY. © 2023 The authors. Published by Elsevier Ltd
The illustration shows heat maps for women, by English district health authority, of the probability for dying from a cancer between birth and 80 years in 2019 (in red), and the change in the probabilities of dying from 2002 to 2009 (in blue).