
The webinar was chaired and introduced by Matti Aapro, Medical Oncologist at Clinique de Genolier, Switzerland, and President of SPCC.
Dr Aapro commented that as the whole world has been hit by the Covid pandemic, we have had to find different solutions for interaction. And even though telemedicine was already in existence, it suddenly became a must in some areas, prompted by fears from patients, difficulties to see the doctor, and vice versa, and miscommunication from the authorities about safety.
Besides the Covid-19 emergency, there are many situations in which telemedicine and digital health can be applied and, actually, can be even preferable to in-person care.
The first presentation was given by Professor Alessandro Stecco, Eastern Piedmont University – UPO, Piedmont Regional Council – President IV Health Commission, in a talk which included the definition of telehealth, and its history throughout the centuries.
What is telehealth?
Although the terms telemedicine, telehealth, and e-health are often used interchangeably, it is best, for clarity, to specify the areas covered by each. The most familiar of the three, telemedicine, means “to cure at a distance.” It comes from the Greek term “tele”, meaning “distance”, and the Latin “medicina”, meaning “cure”. Telemedicine uses technology to remotely deliver care. A physician in one location uses telecommunications infrastructure (ICT) to deliver care to a patient at a distant site. The second term, telehealth, encompasses a wider scope, which includes telemedicine, but also remote nonclinical services, such as preventative and promotive.
Electronic health (e-health) is an even broader term which encapsulates both of the above. E-health can be carried out remotely but also in person and includes all the activities that use communication and information technologies to store, retrieve, share, and exchange health-related information for prevention, diagnosis, treatment, monitoring, educational, and administrative purpose.
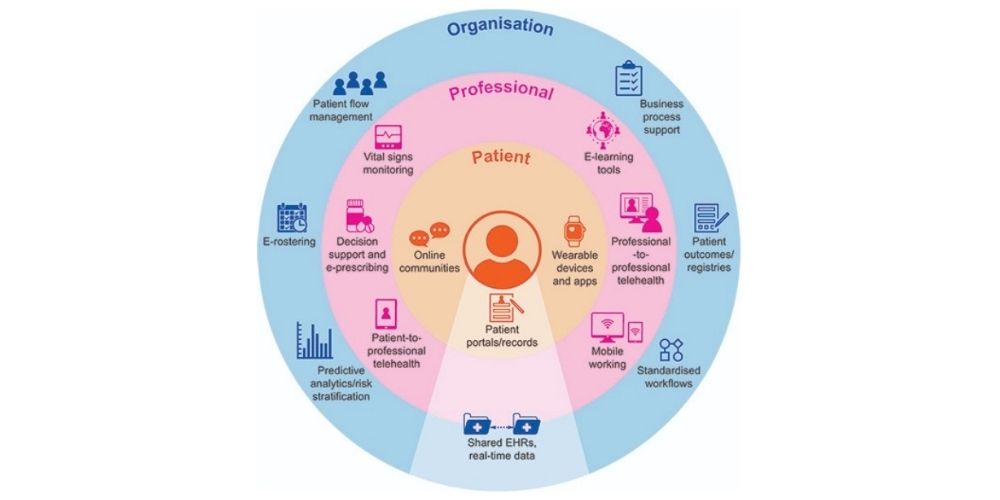
Telepharmacy, teleradiology, telepsychiatry, teledermatology (and many more) form part of telemedicine. Another term that is gaining significance is m-health, which refers to health care delivered and monitored by apps on a mobile phone, tablet, or wearable device. At the centre of the e-health system is the patient, who can improve self-management using apps, online communities, patient portals. Around the patient is the professional and around both is the organisation system, and these three spheres need to work together to function.

Telemedicine is not a new concept. A comprehensive book published in 2009, History of Telemedicine: Evolution, Context, and Transformation by Rashid L. Bashshur and Gary W. Shannon, traces back its roots to ancient societies and their early devices – such as fire and smoke signals – employed to remotely communicate military news or health warnings between settlements. Since the 1900s, inventions such as the telegraph, telephone, radio and television, internet, and space telemetry, have been major drivers in the development of telemedicine. Radiology is one of the techniques that best lend themselves to teleconsultation and telediagnosis.
Not many people know that X-ray remote consultation was tried as early as the end of the 1940s. The first instance took place in Pennsylvania where, after two years of testing, radiologist Joseph Gershon-Cohen and inventor Austin Cooley used a circuit of wire and radio to connect Chester County Hospital to Philadelphia, 28 miles away. The employment of the telegraph in wartime to dispatch transmissions of clinical issues and casualties was also one of the first attempts at telemedicine. Telephone consultations have been used in the past and made a substantial comeback during the current pandemic. The idea of telemedicine was already envisaged in the early 1900s. The Radio News cover from April 1924 depicts a future scenario of “radio doctors” who could remotely cure patients through radio and video consultation. It was still science fiction back then, but it was deemed possible.
In the late 1950s, through to the 70s, the US Public Health Department, the Department of Defence and NASA, invested time and money for research in telemedicine with video transmission of patients, and telemetry to communicate with and monitor astronauts in space. This eventually came to a halt when extramural funding was terminated, and it did not pick up again for almost a decade, until a new and more powerful wave of projects started to develop, first slowly and then exponentially. What happened in the past thirty years in this field is clearly shown in a graph from a recent issue of Connected Health. The percentage of publications on e-health dramatically surged in 2020. Similarly, the number of journals related to e-health has increased massively in the past 20 years, after stalling during the 1990s.

What is needed in the current context
As we had to rapidly learn from the Covid pandemic, three key points need to be addressed: training (both of health care personnel and of patients themselves), interoperability of systems, and patient empowerment. Telemedicine is not fully substitutive of regular medical visits, it must be seen as complementary, a way to fill in the gaps or optimize output in specific situations (remote areas, lack of a specialised resource, stay-at-home policy and so on.)
The latest issue of the Journal of the American Medical Informatics Association concluded that, “While in-person visits are essential in many conditions, telemedicine may be a viable alternative for certain patient population and care needs; understanding and prioritizing patients who are most appropriate for telemedicine and in which clinical situations are important future steps.” Before Covid 19, nearly 90% of EU citizens expected to access their own health data, agreed to share their health data if privacy and security were insured, and to provide feedback on quality of treatments. So, even before the pandemic, the road for telemedicine was already paved.
The Journal of the American Medical Informatics Association proposed some guidelines for telemedicine development and implementation: support secure multidisciplinary consultation and patient monitoring; optimise clinician and patient experience; deploy and optimise ideal care delivery model; embed quality, value, and patient-reported outcome metrics. There are many e-health services currently available (a summary table drawn by Stefano Omboni can be found in the new journal Connected Health).
Setting of application in modern healthcare systems
Telehealth can be employed in a variety of settings: telemonitoring and tele-visit at home; triage from ambulance; tele-reporting and teleconsultation in radiology, and so on; so, it is crucial to create efficient telemedicine settings. Depending on the type of patient and on the connection adopted, solutions can be remote consultation, asynchronous consultation, telemonitoring or tracking. The communication and the transmission tools can be a PDA, tablet, smartphone, laptop, desktop over wi-fi, Bluetooth and so on. The case manager of the patient can be a primary care physician, a nurse, a pharmacist, etc. There is good evidence of clinical benefits of e-health and telehealth interventions in various conditions. Diabetes shows one of the highest, with glycaemic control, but also insulin irrigation in some experimental settings. Heart failure showed reduction in mortality and hospital admissions. Chronic lung disease, arterial hypertension and other chronic conditions also registered some benefits, including cancer, which is becoming an interesting area of development for telemedicine. Mental illness can also get positive results from remote care, as the resources for these kinds of problematics are scarcely available and telemedicine could fill the gap.
Covid ignited the explosive growth of telemedicine, that will likely change the future of healthcare delivery. In the past two years telehealth usage has multiplied. Now we need to understand how to effectively implement it, from the human resources perspective to the importance of connection bandwidth for different uses, and the role that can be played by Artificial Intelligence. There are pros and cons, of course, in telemedicine, and we must understand them to implement this technique in order to help patients receive better care and be more empowered, irrespective of age and circumstances.
Telemedicine in cancer care: an overview
The next presentation was by Andreia Capela, Medical Oncologist, MD Centro Hospitalar de São João Portugal and AICSO Board member.
The pandemic urged on the use of virtual health, and the evidence-based implementation had to be surpassed, there was just no time to publish all the research that was being carried out in the field. International recommendations on the use of telemedicine lack the high level of quality evidence that we would normally expect from organizations such as ASCO and ESMO, but we cannot wait for the evidence to be produced. Virtual care is here to stay, and we must adapt to it, we must engage all the stakeholders, professionals, patients, and caregivers that are using it; also, we must research and monitor its implementation as we do for drugs in phase IV trial. The question is not whether we should use virtual health, but how, where, and when, by whom and for whom. As we know, the patient should be at the centre of care and their needs are paramount. Then we have the health professionals, the caregivers, and the institutions; and around them there is a circle of virtual care, which includes stakeholders not often encountered in oncology or medicine in general, who play an important role in moving telemedicine forward. These are data specialists, informatics, policy makers, marketing and communication, and so on. We must bond with all the new players and look at their reviews and outcomes. We should not only be researching medical journals but also informatics and communication technologies.
Where should we, or where can we use the telemedicine approach? In oncology, we can employ it along the entire cancer pathway, from prevention to bereavement, but we must keep in mind that different approaches are needed at different stages and depending on the different steps taken by the patient. We must obtain better research and implementation; we need to gather more evidence to decide for whom and how telemedicine should be used. The best guidelines and recommendations for oncology come from international societies, such as ASCO, ESMO, COSA. There are also some summary papers that we should consult. Based on the available literature, we can evince that in psychology counselling and monitoring, telemedicine can be equivalent to face-to-face, especially in the case of adjustment disorders. Perhaps, for more complex situations, the in-person approach would still be preferable. Genetic counselling also can be done remotely, literature shows that it is non-inferior to in-person in terms of knowledge, decision conflict, cancer distress, perceived stress, genetic counselling satisfaction. In fact, the delivery mode is more convenient, and the costs lower for both patient and system. Genetic counselling studies suggest that visual cues (body language, expression) available with in-person or video sessions may be better for in-depth counselling, therefore video calls are to be preferred to phone calls. Long term follow-up for asymptomatic patients via telephone yielded high patient satisfaction and proved to be non-inferior for psychological morbidity versus in person follow-up.
Patients’ satisfaction with telehealth can also be associated with the reduction in travel time, cost, and burnout. Studies have revealed high rates of acceptance of telehealth by health professionals (with some technical hurdles and more hesitancy among individuals with less experience). Skin lesions can be evaluated with sufficient diagnostic accuracy through the asynchronous transmission of images, which may facilitate more timely diagnosis with less overload on the physician.
In all, we have sufficient evidence to embrace the recommendation for supportive interventions delivered by phone – and better still by video call for psychology, social work, occupational therapy, exercise physiology, physiotherapy, nutrition, and so on.
Clinical trials can also benefit, as a network of primary and satellite sites can be created. In addition to improving accessibility, conducting trials with this model can help with meeting accrual targets for less common cancer subtypes and improve capacity in the workforce to support clinical trial enrolment.

Contexts of use
In new patient consultations, the remote approach can be preferred, although face-to-face should also be available, if requested by a professional, a patient or caregiver. Second opinion consultations, medication prescription and management, pre-treatment explanation and evaluation, supportive care visit, symptom evaluation and management, treatment monitoring and adherence, psychological evaluation and intervention, survivorship visits, patient and caregiver education, can all be delivered remotely. Also, when a patient has difficulties accessing a clinic, telemedicine can be employed. It can be used for family conferences, allowing everybody who is important to the patient to be present at the discussion. Clinical trials can be explained remotely before consent and signature, and this might encourage more patients to enrol.
For the professional, interprofessional consultation can be more frequent, and access to experts of all specialties will become easier. It is a great opportunity for multi-disciplinary meetings and to reach community services that in many realities are not yet connected to patient care.
When to favour in-person consultation
The initial consultation can be done either virtually or in-person, but it is important to have a face-to-face evaluation of the patient before proposing treatment. For the delivery of key information, such as bad news or a new diagnosis of cancer progression, face-to-face should be preferred. Emergencies and life-threatening situations are not suitable for the virtual mode. Hearing, vision and cognitive disabilities, technical constraints, lack or restricted access to internet, health illiteracy, and poor technological literacy can make remote interactions difficult. Conflict management should also be dealt with in-person, and when there are concerns about privacy. Some patients, for instance, may need help to access technology, and privacy can be compromised that way. In sum, the advantages for the patient are: personal and family empowerment, remote monitoring (via apps and devices), easier and faster communication, better time management, avoidance of distance constraints, presence of important persons, easier referral, access to experts from far away, lower costs, opportunity for clinical trial access, conjoint visits.
As for professionals and institutions, many specialists can be present at one virtual consultation, facilitating multidisciplinary interventions. It can also be an advantage for those medical centres that lack certain facilities. The patients’ status can be regularly monitored within their real environment and daily routines. The costs of transferring patients are lowered. Telemedicine allows more efficient time-management for professionals and better resources allocation. There can be increased collaboration between institutions and strengthening of the connection between levels of care. Telemedicine can be integrated by artificial intelligence, machine learning, remote monitoring, virtual clinics, telenursing, tele-pharmacy, etc.
There are, of course, some disadvantages, such as how to ensure correct physical examination, even with clear instructions. A patient could be assisted in this by local community professionals. Communicating bad news is also a challenge, although there are guidelines on how to do it remotely, a virtual version of the Six-Step Protocol (SPIKES). And we still need to travel to have image and lab tests performed. We are faced with technological challenges and updates, which involve costs and financial investments. There are broadband coverage disparities and lack of e-health literacy. Also, the human touch, the nonverbal communication: it is difficult to show empathy by video, although there are tips on how to do it. There is risk of burnout and stress related to technological malfunctions. There are privacy and confidentiality concerns, cross border regulations, and socioeconomic and demographic disparities that could be exacerbated by technical requirements. Present and future challenges include the need for improved scientific evidence on implementation and outcomes, promotion of (e-)health literacy, engagement of multiple stakeholders, and incorporation of new technology.
We must remember that telemedicine is a complement and not a substitute. E-heath brings huge opportunities in a constantly evolving field. Addressing the gaps in telemedicine should be a continuous process. No one should be left behind. Patient, caregivers, and professionals experience should always be taken into consideration. We must find the optimal balance between in-person and remote consultation. Further research in feasibility, safety and oncological outcomes is needed. Virtual health is a patient-centred care model focussed on connecting patients, families, and providers through technology to promote wellness, deliver specialty care and improve outcomes.

Virpi Sulosaari from the EONS, European Oncology Nursing Society, President-elect, and principal lecturer at Turku University of Applied Sciences, Finland, spoke about Value-based telemedicine in cancer care and person-centred approach.
What is value-based healthcare?
The concept was originally introduced by Harvard Business School Professor Michael Porter. Its central tenet is that the overarching principle in redesigning health care delivery systems must be value for the patient. We define value as the outcomes that matter to patients and the costs to achieve those outcomes. Positive patient outcomes drive costs down in the long run. In the US, value-based healthcare is a delivery model in which providers are paid based on patient health outcomes and satisfaction. Providers are rewarded for helping patients improve their health, reduce the effects and incidence of chronic disease, and live healthier lives in an evidence-based way. There is not quite an equivalent for this in Europe. Also from the US, from the Institute for Healthcare Improvement, comes Triple Aim, a framework focussing on
- improving the patient experience of care (including quality and satisfaction);
- Improving the health of populations; and
- Reducing the per capita cost of healthcare.
One of the means to achieve this is the integration of e-health tools and services in the care system. Care coordination and communication with patients are critical, and telehealth has proven to be a valuable tool, despite the costs associated to the underlying technology. As health professionals our values and aims in healthcare and in cancer care are high quality, effective treatment, supportive care and survivorship support which are timely, accessible for all, affordable, yet tailored for the individual needs of the cancer patient and the caregiver.
What is value-based telemedicine? Telemedicine aims to better the patient experience of care, improve population health, and reduce per capita cost of healthcare, also to improve the experience of providing care. Therefore, it could be seen as a means to achieve value-based healthcare. It is cost effective in relation to the use of health care resources, it allows easy use of PROs (Patient Reported Outcomes), but also it is effective in tailoring symptom management and monitoring, and integrating supportive cancer care and survivorship support. In oncology, telemedicine can improve access to specialized cancer care services, clinical outcomes, safety of care and provision of care, but also the experiences and quality of life of people affected by cancer, and reduce their symptom burden. Cancer patients often require a close and continuous connection to the multi-professional team responsible for their care, as well as efficient communication channels. Telemedicine can offer time-sensitive connection without compromising quality of care. For the multidisciplinary teams, telehealth technologies offer opportunities to track and monitor the care across the cancer continuum, it allows timely reaction on care needs and early detections of complications. It also provides channels for interprofessional communication, information sharing and clinical decision support. Jennifer Bauer, expert in data privacy and cybersecurity, has proposed a holistic approach to e-health services that combines technology, digital expertise, and clinical experience, and empowers physicians and care teams to communicate more effectively with their patients, shape engagement strategies that drive targeted behavioural change where needed, reduce unnecessary healthcare expenses and inefficiencies in care management practices, and improve the results of chronic condition and disease management programs.
Many telehealth services provided by oncology subspecialties are healthcare professional to healthcare professional, or, for example, technology used in radiotherapy treatment planning. We also have e-health or telehealth services that connect healthcare professional and patient, such as patient education, or allied health professionals who support and educate cancer patients or provide a swallow assessment or conduct psychosocial counselling. Among the positives outcomes for the patient are reduced travel and travel costs, and the opportunity to concentrate on trying to live a life as normal as possible. There are many information and communication technology-based solutions for people with cancer. Some examples are platforms, devices, and mobile applications (m-health) for self-management, symptom management, life-style modification, medication adherence, delivering real time data on a patient’s health condition (e.g., wearables), and storing personal health information.
Person centred care approach
An important aspect of cancer care and telemedicine is patient-centredness and how this can be supported through the application of technological advances. Person-centred care helps health care professionals to better understand people’s individual, unique, experiences, and tailor the care to their needs and preferences. Following the definition given by the Health Innovation Network, “Person-centred care is a way of thinking and doing things that sees the people using health and social services as equal partners in planning, developing and monitoring care to make sure it meets their needs.” We need to consider desires, values, family situations, social circumstances, and lifestyles of our patients, and see them as individuals. As professionals, we are there to empower our patients and accompany them on their journey in the cancer care continuum. Care services need to be more flexible to meet the patient’s needs in a manner that is best for the patient. This should also be true in the development of telemedicine in oncology. However, the adoption of telehealth technology relies on patient participation and the motivation of patients to become partners in their health care. So, telehealth promotes a shift to a more participatory care and an improved health system driven by patient empowerment.

The development of telemedicine with a person-centred approach requires evidence: do we have it? Of course, more research is still needed, but a quick search on PubMed, limited to systematic reviews published in last 5 years for “((telemedicine) OR (telehealth)) AND oncology” yielded seventy-four results and with limit to “patient-centred” three, showing that there is already a lot of information available. We have for example information on recent developments in e-health and m-health to manage cancer and other chronic diseases. We have information on the perspective of cancer patients at the rapid implementation of telemedicine during the Covid-19 pandemic. We have information about methods such as telephone interventions for symptom management. We have information from different patient groups, also evidence on different symptoms, on quality- of-life of cancer patients, mobile health applications, and so on.
To successfully implement telemedicine, clinicians and cancer patients alike need to be able to trust the system. We need to ensure privacy, confidentiality, and security in digital health care. For the person with cancer and their informal caregivers, we need to know what kind of information and support they need and at what point of their care. We need to ask patients and caregivers their experiences and carry out feasibility assessment. We must provide education and simple enough user instructions, and provide alternatives. Elderly people, for instance, may not have the skills to use all the apps currently on the market. For the clinician, there needs to be an evidence base, involvement in the development process, education and training, clear and systematic implementation models, etc. The outcome evaluation is important, we need to evaluate whether we have achieved what we were aiming for.
During the COVID 19 outbreak, we have learned to use more and more efficiently digitalised tools in health care from simple information technology solutions to more complicated monitoring and symptom assessment tools. We have also gained a lot of experience, so we need to learn from this experience, and we have the information to help us use telehealth to deliver better care for people affected by cancer.
The final speaker was Robin Zon MD from Michiana Hematology Oncology’s Advanced Center for Cancer Care, and Co-Chair of ASCO Telemedicine Standards Expert Panel
Patient’s Perspective in Digital Health
Telemedicine has been used for a long time, but variably, in the US. The Center for Medicare and Medicaid Services (CMS) established when telemedicine could be utilised and was quite restrictive for many sites across the country. Michiana Hematology Oncology (MHO) is a community practice with six sites of service across Northeast Indiana. MHO doctors are not employed by any hospital or academic institution. Due to CMS existing regulatory language regarding geography, even though MHO doctors wanted to use telemedicine, they were unable to do so. When Covid was declared a Public Health Emergency in the US in March 2020, CMS loosened their restrictions. The new regulations were announced on a Friday afternoon and by Monday morning, MHO had a HIPAA compliant platform in place to be able to access their patients. Early in the pandemic, in the pre-vaccination days, doctors still went to work every day and saw their patients in hospital or in their practice, but in the practice, visits were limited to infusion patients or emergency symptom management in-house. Everything else was dealt with by visual or audio. For the first year, 2020, about 70 to 80% of visits were telemedicine based. Some of the older doctors who were more at risk were using telemedicine more than the younger doctors. But as vaccinations were offered, use of telehealth decreased, and now it comprises less than 10% of total visits, but it is still very useful. Overall, patients were, and still are, very thankful to use telemedicine. They were able to avoid unnecessary travel and exposure, and initially, during lockdowns in the US, people were not allowed to go out, unless for absolute necessary reasons, including healthcare. Masks in the US were difficult to find, the elderly were advised to stay indoors, and transportation was a problem. Currently, telehealth is very helpful for symptom control as well as drug management. And it limits the time away from work, which is important for younger patients. It has reduced no-show rate and is especially useful for those who have transportation or childcare issues. Initially, doctors used audio/visual quite frequently, while now they are using audio more.
ASCO invited a number of oncology clinicians to fill in a survey on telehealth utilisation patterns, preferences for telehealth utilisation after the pandemic ends, and perspectives on barriers to telehealth and cancer disparities. Although only 200 individuals responded, it is possible to evince from their answers that frequency of use and perceptions of quality varied by type of visit. Most clinicians plan to make use of telemedicine in the future, but commonly they reported barriers to telehealth that increased cancer disparities. For instance, in the US, broadband is not always accessible, especially in rural communities, but even within cities, some people may lack the money to attain internet and broadband. From the provider perspective, there emerged that telehealth is better or similar to in-person for survivorship visits, consent visits, and symptom management, but is not as appropriate for new patient visits or for discussions regarding end-of-life care or hospice.
The patient perspective
The Patient Advocate Foundation (PAF) is a US non-profit organization founded in 1996, which provides case management services and financial aid to those with chronic, life-threatening, and debilitating illnesses. In its 25 years of existence, it has helped more than 1.6 million patients nationwide. The CEO, Dr Alan Balch, sent out a survey by email to over 15,000 patients in the time-period between May and July 2020.
The respondents may have had a diagnosis of COVID-19 in their household or were impacted by quarantine or pandemic measures. There was a 27% response rate, which is quite high. As to the overall demographics, more women than men answered the survey, the ethnicity reflected pretty much the usual population in the US, with mostly Caucasians answering, followed by African American, Hispanic, and then others.
The income group was primarily less than 72,000 US dollars. The age group was primarily less than 75, not a surprise given that many 75-year-olds do not have email.
As to location, suburban was nearly half of the respondents, but there were good numbers of urban as well as rural. Education level was up to some college degree with also some graduates. The region that was most represented, over 50%, was the South. When it comes to insurance and carrier, they were mostly Medicare and Medicaid.

Since the start of the pandemic, 50% of the respondents had completed between one and two telehealth visits, a few had over five. The types of healthcare services delivered during these visits were mostly for routine follow-up as well as drug management and reviewing results from tests. 0% of patients reported end of life care. 80% said they were extremely or somewhat satisfied with the level of virtual care they received, while 2% were dissatisfied. Most patients felt that non-routine visits for existing treatment, or for symptoms suggesting new diagnoses, were not something that they would prefer telehealth for, favouring face-to-face instead.
Telehealth in Oncology: ASCO Standards and Practice Recommendations
In July 2020, ASCO issued an interim policy statement on telemedicine, which encouraged policymakers to permanently expand coverage and to adequately reimburse providers for telehealth services. Providers and patients have reported that telemedicine has many benefits, including easier access to care, but concerns have been raised about privacy, adequate reimbursement, lack of infrastructure, and inequity. Following the publication of ASCO’s interim statement, the subsequent ASCO Road to Recovery Strategy identified a need within the ASCO membership for more detailed oncology-based standards. The ASCO Standards and Practice Recommendations were created in response to this need and include a systematic review of current evidence for different methods of telehealth delivery in oncology. They also provide oncology specific standards on topics such as selection of patients and multidisciplinary cancer conferences. The systematic review addresses questions such as: outcomes for patients seen via telehealth vs. outcomes for patients seen via in person visits; which patients should be seen via telehealth vs. in-person; oncology specific workflow and other implementation considerations; standards for establishment of the physician/patient relationship in context of telehealth and oncology; expert panels guidance for when a patient may see an advanced-care practitioner in person, such as nurse practitioners, physician assistants, or by telehealth visit; the role of allied health professionals in oncology specific telehealth interventions; discussion of patients at virtual Multidisciplinary Cancer Conferences (MCC) feasibility compared to in person MCC meetings; and how telehealth can be incorporated into clinical trials in oncology.
Future Research
High quality research is needed across all areas of telehealth, and there is a gap in published research on telehealth in cancer survivors. More detailed reports are needed on how the response to electronic symptom reporting is organized and incorporated into workflow. There is a need for more data on patient-centred outcomes and long term follow up for all populations, including how telehealth can assist in eliminating barriers to care. Future analysis must consider private versus government payers. Interventions are often multi-faceted, and more research is needed to determine the individual effects of different intervention features. Best practices should be identified and disseminated to raise the bar for telehealth performance. More consistent terminology should be adopted for interventions and definitions of outcomes, to facilitate comparisons across studies and syntheses of findings.
Telehealth is meant as an adjunctive care strategy in the overall care management plan for delivering best care for the patient. Altogether, patients appreciate the service of telemedicine, but they should always be given the option between in-person or telehealth visits according to personal preference. The patient preference should be driving the utilization of telehealth, provided there are no other restrictions in place that are external to the provider-patient relationship. Practices should develop policies procedures that outline preferred frequency of telehealth versus in-person visits during the cancer care continuum and consider patient preferences.
Next Event










