Chair of the webinar in the SPCC series on Improving Efficiency in Cancer Care, was Prof. Dorothy Keefe, CEO of Cancer Australia.
One of the main problems in Australia is the inefficient way cancer care funding is dispensed. If it were used more efficiently, a lot more could be done for the patients, Prof Keefe explained, before giving the floor to two qualified experts in the area of value effective care, Professor Jeff Dunn, from the Prostate Cancer Foundation of Australia and President Elect of UICC; and Professor Christobel Saunders, from the University of Western Australia, and active member of All.Can.
A community perspective of efficiency in Cancer Care
Prof. Jeff Dunn, AO, CEO of PCFA & UICC President-Elect
Professor Dunn opened his talk by quoting Will McDonald, a well-known Australian journalist who was diagnosed with prostate cancer at age 42, only six months after his father was diagnosed with the same, “So much heartache we can avoid by improving the way things are done.”
Improving cancer care is not all about economics, or making sure that the system runs smoothly, it is about producing outcomes for patients.
According to the Australian Institute of Health and Welfare (AIHW) 150,000 Australians are diagnosed with cancer each year and around 50,000 will die. 1 in 2 will get cancer by age 85.
It is important to remember that cancer is not a single disease. There are 90 different disease classifications, and 130 cancer medicines are listed on the Pharmaceutical Benefits Scheme (PBS). It is a complex scenario: different symptoms, different treatments, different impacts.
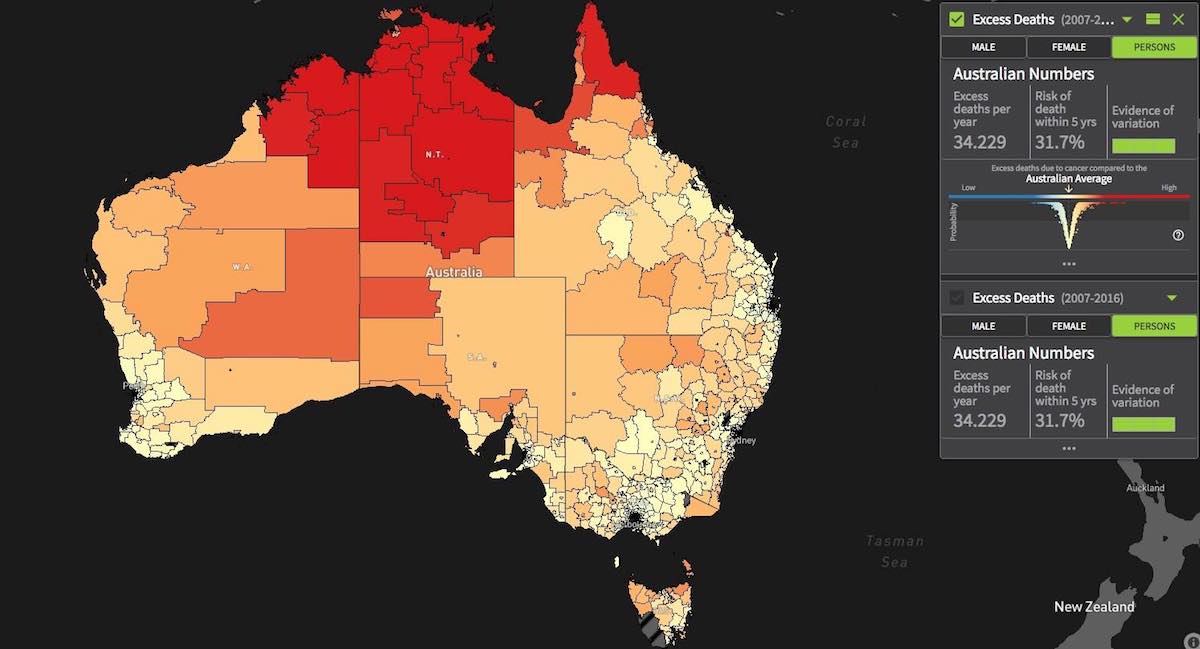
By world standards, Australia has an efficient health system and one of the highest cancer survival rates. The most diagnosed cancers in men are prostate, melanoma, colorectal and lung. And in women, breast, colorectal, melanoma, and lung cancer. The survival rate for all cancers has increased from 51% to almost 70% in the past two decades. For some cancers, like breast and prostate, a five-year survival rate is as high as 95%. But it is difficult to efficiently share the gains and benefits equally across the whole population. The more rural areas, for instance, have much higher excess deaths from all cancers. There are geographical, socio-demographic, socio-economic, and health system differences that need to be considered.
Australia has a subsidized health system. The expenditure on health has grown greater than the rest of the economy. It represents about 10% of the gross domestic product, while the OECD average is 8.8%. Improving efficiency is not only important in terms of health outcomes, but also of affordability. Of the almost $200 billion spent a year, most go to hospitals, closely followed by primary care. In a pie chart of the expenditures, not even a thin slice is directed to preventive health and health promotion. As it is possible to prevent certain cancers and downstage their diagnosis through early detection, changes in the way the work in cancer care is funded would be beneficial.

Why is the community sector so relevant?
In Australia there are 4200 healthcare charities, which employ over 300,000 staff and contribute about $19 billion annually to the healthcare sector. Non-government organizations provide an essential function in the delivery of community-based health promotion and care coordination, programs that enable informed decision-making, improve patient-clinician communication, and the empowerment of personal agency. Community organizations establish a common debate, to try and fill gaps, innovate, and strive to improve outcomes for people. When we talk about efficiencies in cancer care, an important part of that discussion may well be about how to acknowledge the contribution from the community sector, and then, go about coordinating it. Because it is indeed an extensive contribution. How to harness that community energy? How to direct it? To quote the definition given by S. Palmer and D.J. Torgerson, “Inefficiency exists when resources could be reallocated in a way which would increase the health outcomes produced.”
Are efficiency and quality mutually inclusive?
Quality and efficiency may be evaluated differently from different perspectives. Patients might view quality through the lens of their own individual needs, i.e., access to doctors, services, and treatments that maximize their ability to work and enjoy life. Health professionals may see it as their ability to exercise medical mastery, in order to cure and provide best treatments and outcomes; while the public health system might look at quality and efficiency as an improvement of statistical outcomes, i.e., high levels of access to primary care, low morbidity, and mortality rates. Of course, there may be tension at times between the different perspectives. The challenge in improving efficiency is to make the most of that tension and to turn it into positive energy, by encouraging collaboration.
How’s Australia currently performing?
The national-level findings for Australia from the All.Can international patient survey show that delays in initial diagnosis, and managing ongoing side effects were identified by respondents as the biggest causes of inefficiency. 50% of respondents reported not receiving enough support to deal with ongoing symptoms and side effects. One in eight respondents, whose cancer was detected outside of a screening program, waited over six months to be diagnosed. And 41% of respondents reported not receiving sufficient information about signs and symptoms of their cancer returning or getting worse. Although there is a terrific health system in Australia, there is still plenty of room for improvement. 20% of all health expenditure is currently wasted on ineffective practices, and two or more years of life expectancy could be gained by reducing inefficiencies.

Understanding efficiency from the patient’s perspective
When we talk about efficiency, we must put the patient’s voice at the centre. To give an example, in 2020, a multi-disciplinary expert panel was brought together to better understand the nature of prostate cancer survivorship in the Australian context. Seven priorities were identified:
- Better patient clinician communication
- Developing a survivorship toolkit
- Increasing access to multi-modal care
- Reducing out-of-pocket costs
- Promoting the uptake of exercise
- Harnessing technology
- Greater reach of specialist nurses
“Prostate cancer survivorship essentials framework”, by Jeff Dunn et al., was recently published in the British Journal of Urology International. Six key domains are pinpointed: health promotion and advocacy; shared management; vigilance; personal agency; care coordination; and evidence‐based survivorship interventions. But again, the central element, right in the middle, is personal agency.
A coordinated and evidence-based approach to cancer-control is essential, all the players need to work together and to collaborate to ensure an evidence-based approach that can be pursued as a collective. Perhaps the ultimate measure of efficiency is the value it returns in terms of quality-of-life to individual patients.
Prof. Keefe agreed on how important it is to refocus on the patient agency as the centre, before introducing the second speaker.
Efficiency in cancer care: an Australian example
Prof. Christobel Saunders AO, Professor of Surgery UWA; Consultant Surgeon; Director Breast Cancer Research SJoG Subiaco Hospital; Chair PathWest Laboratory Medicine
The definition of efficiency formulated at All.Can is that efficient cancer care delivers the best possible health outcomes, using every tool available, human, financial, infrastructure, technological resources, but the best outcomes are the ones that really matter to patients and to society. Interestingly, that has little to do with what doctors or health systems think of as efficiency. For cancer patients, inefficiencies lead to premature mortality, reduction in quality-of-life, financial and time losses, and inequities between different groups in society. By reducing inefficiency in cancer treatment, two to six years of life could be gained. Around the world, inefficiencies weaken health systems by more than a trillion dollars a year. Around 20% of all health expenditure is wasted on ineffective or inefficient practices. As Professor Dunn pointed out, the Australian health system has achieved some great outcomes, but it is expensive, it is one of the highest in the OECD. And the costs are increasing year on year. There has been progress in many areas, life expectancy has improved dramatically over the past decades, as indeed disability adjusted life years. People are smoking considerably less and drinking less. Despite this, chronic health challenges continue to grow. The chronic health challenges of lifestyle changes that lead to obesity and lack of exercise, and indeed cancer, which is growing at a significant rate each year.

How to achieve better efficiency in cancer care
As Professor Dunn clearly stated, to put the patient at the centre is fundamental. The patient perspective should be the main determinant when defining health outcomes that matter. But to achieve this, it is necessary to scale up good practices: champion efficient and innovative cancer practices and retire ineffective ones; to break down silos, foster a collaborative approach across the entire health system; good technology: invest in digital innovations, assess and adopt diagnostics and digital tools that improve health outcomes; and support healthcare staff across the sector. A joint effort is required, from public and private health systems, patients’ families, and carers. The charitable sector also has an important role to play. It is crucial to consult with patients and their carers to find out what they need, in order to design a value effective care model, and then implement it into clinical practice. Other goals: avoid unnecessary interventions, improve early diagnosis and treatment. And, most importantly, implement a value-based healthcare model, where value is defined as the health outcomes that matter to patients over the cost of delivering those outcomes. This should result in several benefits for patients such as, for example, reduction in out-of-pocket expenses and improvement in health outcomes. But it should also result in a more cost effective and efficient system.
So, what do patients say their issues are in cancer? As shown in the survey carried out by All.Can, patients want an efficient diagnosis, joined up seamless care, good psychosocial support, and they also want to understand the costs they will encounter. Out of the $185 billion Australia spends on health care a year, about 17% are out-of-pocket expenses, largely driven by surgery, diagnostic imaging, and, in the case of cancer, by radiotherapy. Costs vary greatly depending on what provider the patients use and where they live. There is huge inequity, and a great lack of transparency around this area.
The model that is being worked on in Australia by the CIC Cancer Project is that of bundled care. In the case of breast cancer, which is only second to prostate cancer as the highest costing, a Coordinated Care Model in breast cancer is being devised, based on a partnership between private health providers and health funds. The first step of the project was to delineate a pathway of care in early breast cancer and then accurately cost it. This was done for the private sector but can be adapted to the public sector as well. Every step of the pathway was assessed, and the best care established. These bundles of care are being developed, making all the costs transparent. There will also be a navigator on board, who will lead the patient through the extremely complex Australian health system, lowering distress levels. The goal is to achieve quality value-based choices for patients with breast cancer. Once successfully tested in the small number of centres where it is being trialled, this system can be replicated and scaled up, perhaps, to other cancers, and other institutions. GenesisCare, a private radiation oncology provider, have taken the lead in this, also shouldering the financial risk by capping out of pocket contribution. So, should there turn out to be some big outliers, it will not be the patient who pays, but GenesisCare. The ideal scenario would be to have a complete $0 out-of-pocket expense for a patient going through the private system, but that is proving difficult. So, a cap is the best next thing. The insurance and GenesisCare pay for the entire cost of the first year of the pathway. After being diagnosed with cancer, patients see their first provider, usually a surgeon, and then continue along the pathway of care, surgery, radiation, oncology, chemotherapy, but also, all the supportive care, such as physiotherapy, dietitian, psychological support, and so on. After careful calculations, the proposed cap was set at $2,000. For most patients going through the private sector, this should mean saving money. And in fact, they will only pay for the services they use. So, if they use less services than are in the bundle, they will pay less.
The idea behind bundled care is to provide excellent, navigated care, support and treatment as needed, including supportive care, and at a known upfront cost. This should provide cost savings for the patient and ultimately for the health system because it can build efficiency into the system, and also reduce the psychological and physical trauma of having cancer, through knowing what to expect.









