The session was chaired by Marlene Thomas, Global Medical Lead for Integrated Health Care Solutions at Roche Headquarters. In February 2021, Europe’s Beating Cancer Plan was launched. The plan takes a very holistic approach to the patient journey as it covers cancer prevention, early detection, diagnosis, and treatment, as well as quality of life and survivorship. It presents a unique opportunity to improve and evolve the way oncology care will be delivered in future. We need to make sure that healthcare systems are ready to take on innovations such as advanced diagnostics or digital health solutions, artificial intelligence-based algorithms, as well as new drugs and therapy concepts, so that every single patient can benefit. Of course, every Member State deals with different challenges, therefore, we need to accommodate healthcare system diversity. The EU Beating Cancer Plan can help to architect a future-proof and patient-centric care delivery pathway. This requires collaboration across the board. Academia, industry, government, all having a seat at the table to design new paths to clinical care and explore more collaborative approaches. For instance, Roche recently joined the Optima IMI project, which aims to tackle cancer through real-world data and AI. OPTIMA is a great example for bringing public and private partners together to jointly create and develop a scalable and regularly updated guideline decision-support solution for breast, lung and prostate cancer. In the past two years it has accelerated collaboration beyond borders, and there is much more we can do to work together towards more efficiency, access to data and innovation.
Regions: a bridge between policies and practices
Giovanni Gorgoni is CEO at AReSS Puglia, the regional government agency for health and social care innovation for the Puglia region, in Italy, and Chair of the European Regional and Local Health Authorities (EUREGHA) in Brussels.
Before delving into the regional perspective, Dr. Gorgoni summarised the main points of the European Beating Cancer Plan. The plan is made up of four stages, covering the entire cancer care journey. It has ten flagship initiatives and multiple supporting actions to implement innovation and technology in the approach to cancer, sustainable cancer prevention, early detection, quality standards in cancer diagnosis and treatment, and quality of life for cancer patients and survivors. The initiative to reduce inequalities is aimed both at Member States and regions.
You get what you measure: what do you measure?

The European Beating Cancer Plan is the latest of a long list of initiatives (more than 20) launched since 1985 by the European Union with the Europe Against Cancer Program. It is also the most structured and better funded: 4 billion euros coming from EU4Health, Horizon Europe, Digital Europe Program and Erasmus Plus. But are 4 billion enough? Unfortunately not, especially when compared with the direct costs of cancer in Europe, which in 2018 was over 100 billion euros. It is, however, a good starting point. Together with other funding interventions from the EU it can be implemented and integrated by the discretional intervention of Member States and regions. You get what you measure. We measure money, but we also measure epidemiological figures, incidence, mortality, survival, and prevalence rates. If we look at the mortality rates between countries, we see big differences, but there are even bigger ones between regions in the same country. How aware are we of this?
Regions: a bridge between policies and practices
Regions can be an important bridge between policies and practices. For example, one of the flagship initiatives of the European Union Beating Cancer Plan is Better Life for Cancer Patients. This initiative will need macro-level intervention from the EU/State in terms of policies, funding, standards, guidelines, auditing, procurement, to then arrive to the community/patient level: healthcare providing, process integration, outcomes achievement, education and training. There is a missing step, however, that could be covered by the region, in terms of population health management, regional network designing, sub-funding and procurement, education and training, and auditing too.

A “value” proposal
EUREGHA’s proposal for regional level implementation as a bridge for the European Beating Cancer Plan derives from the concept of value-based healthcare (VBHC), proposed years ago by Michael Porter. Porter’s value agenda consists of six main components:
- Organize into integrated practice units (IPUs)
- Measure outcomes and costs for every patient
- Move to bundled payments for care cycles
- Integrate care delivery across separate facilities
- Expand excellent services across geography
- Build an enabling information technology platform.
What is the challenge? The challenge is always to solve the difficult equation between the value that any health organization should pursue, the outcomes that matter for the patient, and the costs to achieve those outcomes. There are two paths that every health organisation can take, both starting from the organisation into integrated practice units: an integration path, or an outcomes path, implementing systems of outcomes and cost measurement, and bundled payment. The sixth step, “Build an enabling information technology platform”, underlies all of the steps.
A showcase of best practices from EUREGHA members
A booklet was released last month with examples of nine best practices from EUREGHA members (downloadable at http://www.euregha.net/wordpress/wp-content/uploads/2018/11/EUREGHA-Booklet-on-Cancer.pdf). The first example comes from Apulia, Italy, where Dr. Gorgoni is based: a regional centre of telemedicine created to digitally enable the personalised care processes for cancer patients with complex conditions. The following two examples, also from Italy, come from the Emilia Romagna region. The first is a network of 12 “Breast Units”, a component of the wider regional cancer network, the second is a multi-stakeholder oncologic drug governance. This regional working group has the task of drawing up evidence-based recommendations that systematically identify for each cancer type, for each line of therapy, and for each patient, the best treatment in terms of risk/benefit and cost/opportunity ratios. Another example, this one from Lower Austria, is the Oncology Information System (OIS). The OIS is a comprehensive tool for organising and documenting oncological patient data. It is a daily working tool for physicians in all 27 hospitals in Lower Austria. From the Flanders comes the Study NOOIT (NEVER), a special program to detect and rescue those women who never responded to an ordinary screening program for breast cancer. An example from the Skåne county is the National e-library for standardized chemotherapy regimens. The Regional Cancer Centres (RCC) in Sweden have developed a national e-library containing around 600 chemotherapy regimens. The primary users are physicians, pharmacists, and nurses. Two more examples from Italy: Tuscany has a multidisciplinary and integrative approach to cancer patients and disease. Healthcare pathways for cancer patients are integrated by evidenced-based complementary medicines that can be used for the treatment of the symptoms of anticancer therapies, as a supportive care before and after surgery, during and after chemotherapy, during hormonal therapy and radiotherapy.; from Veneto is the Institution of Veneto Oncology Network, a regional network structured in the following levels: coordination of Veneto Oncology Network; Veneto Oncology Network Scientific Committee; Reference Hubs; Clinical Oncology Departments and Multidisciplinary Oncology Teams. The final example is from Wales, with the Quality Statement for Cancer, a policy for cancer services which identifies 22 quality attributes for cancer services, with a particular focus on consistency of services across the country.
All of these nine best practices concentrate on a value agenda of integrated practice units, excellence of geographic clinical networks, outcome measurements, and information/communication technology, to enable a smarter, more efficient, clinical process. This is EUREGHA’s concrete proposal to draw the European policies into regional local practices. Because, more than ever, at the centre of the next new normal is community. And the region is the closest embodiment of the concept of community.

Harnessing Data: An Urgent Priority in Cancer
Vivek Muthu, Managing Director at Marivek Healthcare Consulting, in London, took as a basis for his presentation the policy report published by All.Can, Harnessing data for better cancer care. There is a serious issue with the financial sustainability of cancer care. This is not a post-COVID or an intra-COVID situation, but something that has been building across all areas of healthcare for the last 20-30 years, and it is a particular issue in cancer care. Improving data infrastructure, access and use of data is the only way to ensure sustainability. Often, when citizens or politicians are asked what is important in cancer care, they may speak of pharmacotherapeutics and advances in biotechnology. Of course, these are very important, but investing in data infrastructure is equally important. Data saves lives: it is a frontline clinical intervention. Data collection, analysis and use is our responsibility, as citizens, patients, and clinicians. It is an important responsibility, and an urgent one.
Our health systems and cancer care systems are in crisis and have been so even before the pandemic, because of rising costs, and long life expectancy – which, incidentally, is a testament to the success of our health systems and welfare states. We live longer, often with chronic comorbidities, which makes us prolific consumers of healthcare resources. There is rising demand and expectation, perhaps rightly so, among populations, regarding health and wellbeing. But, for how much we might invest in expensive technologies to improve our health, because we have already done so well, there are diminishing returns. There is a sort of cap on how much we can extend our lifespan and wellbeing. And so, overall, interventions deliver diminishing returns. There is a cost and quality crunch within our health systems, including cancer care, which we must bear in mind.
Waste in health systems
Unfortunately, there is a lot of inefficiency in our health systems. Inefficiency sounds like a cold term used by bureaucrats and technocrats, but in the context of care, it translates into lives lost unnecessarily. Waste happens in the form of ineffective or harmful interventions, overuse, inappropriate use, preventable complications, unwarranted variation in practice, duplication, wasted and missed consultations, care discontinuity, poor resource allocation. Out of the hundred billion euros expenditure in cancer care, mentioned before by Dr. Gorgoni, we can expect that perhaps 20 to 40 billion is actually wasted. The figures for avoidable harm alone are rather frightening. Across the whole healthcare, not just cancer, studies report that in the U.S there are between 150,000 and 400,000 preventable deaths as a result of hospital care annually. Four to eight million people are seriously harmed. Figures in the UK also tell a story of avoidable harm, and the problem is certainly not unique to these countries. This is what inefficiency actually means when talking about healthcare.
Root causes
Cancer care, of course, is based on evidence and clinical trials, but if there is no systematic real-time tracking or analysis of health needs, care processes and outcomes, it is almost as if we are throwing resources into a black box.
Epidemiology, as was mentioned earlier, is often patchy. We do not know what input resources (costs, time, workforce) are going in. We do not capture in high-definition citizen and patient characteristics or all the processes and interventions that a patient will experience; and outcomes are not captured systematically. Which seems odd, given that the main purpose of healthcare is to deliver good quality outcomes. But all of this can be addressed. The technology is there and, provided there is the will and investment, it can be rolled out at scale.

“Pull” factors
The use of data won’t just help us solve today’s problems; it will also get us to another level. Advancing science and technology, biotech interventions, personalisation, care specialisation and configuration, all require better data systems. Genomics, for example, will see decreasing operational costs – Moore’s Law applies. The advancement of technologies to analyse genomes, not just for single gene mutations or fusion products, will result in improved therapeutic approaches. Prevention and patient management will improve. The revolution that we are just starting is equivalent in its impact to the germ theory of disease. The journey we are embarking on in cancer care is going to require data en masse and the ability to analyse it. This is what personalisation means. It is not limited to genomics, it includes the ability to capture in high definition everything to do with the patient, to analyse it in aggregate, and then use it for the individual patient. These systems of complex care will necessarily require increasing consolidation of some types of care into specialist centres. We need to be able to configure such centres, including the way in which peripheral centres will feed in and receive information from, in order to deliver care at local level. We will also need data systems to improve continuity and to enable that care configuration. Finally, our R&D processes are missing out on important data. Cancer care systems are seeing millions of patients all the time, and that data should be captured to drive research, development, and innovation. Research happens in clinical trials and leverages the clinical centres, but real-world data could be captured from every single interaction, because it will make for efficient R&D, and help reduce some of the rising costs in all the services required for good quality cancer care. This is the sort of holy grail of what a data enabled health system would be like. Capturing epidemiological data, patient data, in terms of health record, risk factors, other phenotypic data, investigations, including genomics, and imaging, pathology, et cetera. Processing data, what happens to patients when, and then mapping those against the outcomes, so that physicians can assess whether what they are doing is delivering good quality outcomes for patients, or where the gaps are, and where the unwarranted variation is.
As shown by findings from All.Can and other organisations, often patient reported outcomes overlap only partially with what healthcare professionals are currently recording as outcomes in clinical practice. We really need to be focused on what is important to patients. And then there is cost data, which is required in order to make the most of those precious resources we are putting into cancer care. That has to be processed by machines as well as humans. Data have to be aggregated en masse. And the more data there is, the more it is shared, the better outcome and the higher resolution the insights will be. This will lead to better knowledge about diseases, about different cancers, and what is needed to treat them. Data needs to flow between different segments of healthcare. This will improve continuity, and help to derive better evidence-based policy around cancer control prevention, screening, diagnosis, management, and all the psychosocial aspects of care as well.
Challenges
There are many inherent challenges. Data can be messy and poorly captured. There can be challenges with the data systems and how the data can be linked across different systems and the interoperability of those systems. And then there are human challenges, such as low patient trust in the appropriate use of their health data or privacy protection. And then high burden of data collection, leading to limited buy-in from healthcare professionals. There are also challenges around drawing insights, inadequate analytical methodologies, poorly validated artificial intelligence algorithms and inherent biases with data analysis. Any intervention in healthcare has benefits and harms, and we must make sure that the way we are using the data results in more benefit than harm.
How to get there
A basic framework model to get there with data in cancer care systems must start with setting forth overarching principles and values – values around equity, ethics, data governance, data transparency. This needs to be supported by policy and regulation around data and data analytics. We need investment in the data infrastructure and to build it where it is still not present. We need to enhance the capability and engagement of both citizens and professionals, and we need technical standards. The Open Data Institute has been looking at the use of data in health systems in Europe. A paper was published recently, looking at where different Member States are in terms of their focus, willingness, and openness to invest in these areas.

European aspirations
Landscape initiatives: Above the specific initiatives relative to cancer care sits the larger framework of landscape initiatives not just for healthcare, but across all sectors of the European Strategy for Digital Europe, including data governance and technical standards.
Health system initiatives: In the area of digital transformation of health and care, there are initiatives such as the European Health Data Space, Pharmaceutical strategy for Europe, Darwin EU (Data Analytics and Real World Interrogation Network), 1M+ Genome Initiative, and the European Reference Networks (ERNs).
Cancer initiatives: European Beating Cancer Plan, EU Mission on Cancer, Cancer Information System, European Cancer Imaging Initiative, are all initiatives focussed specifically on cancer, but we must remember that they cannot be divorced from the health system as a whole, the two must work closely together.
Financial commitments
These initiatives are complemented by financial commitments at EU level. We can argue about whether those financial commitments are adequate, but we must not forget that this is a movement that involves both public and private sectors. There is a massive private sector investment and innovation in data and digital health. It might not always be perfectly aligned with the EU aspirations, but it certainly contributes to the investment in and promotion of data. There are also external societal drives towards data and digital transformation, which we have seen accelerated through the pandemic. The response to the pandemic would have not been nearly as effective without the real-world data collection and the digital services that have been rapidly put in place to support our health.
Data is a critical resource for health systems: it is the only way ahead. It is the key to sustainability, the key to keeping a universal health system that delivers care to our populations equitably. Providing data to support population health is a civic and clinical responsibility for everyone, irrespective of the hat we are wearing. Data saves lives – it is a frontline intervention. We must take it as seriously and promote it with the same ardour that we show for other critical medical interventions.

Driving for efficiency in cancer care through effective patient pathways
The last speaker was Simon Oberst, Director of Clinical Development at the Cancer Research UK, Cambridge Centre; Chair of the Accreditation Board, Organization of European Cancer Institutes (OECI). The cancer care pathway is the complex intervention for the mutual decision making and organisation of care processes for a well-defined group of patients during a well-defined period. As such, it includes all activities from symptom onset, through diagnosis and treatment, to follow up, to survivorship or palliative and end of life care. It includes the logistic management of care processes from primary care referral to an outpatient clinic, a day care unit, diagnostic processes, treatment processes, inpatient, radiotherapy, supportive care, et cetera.
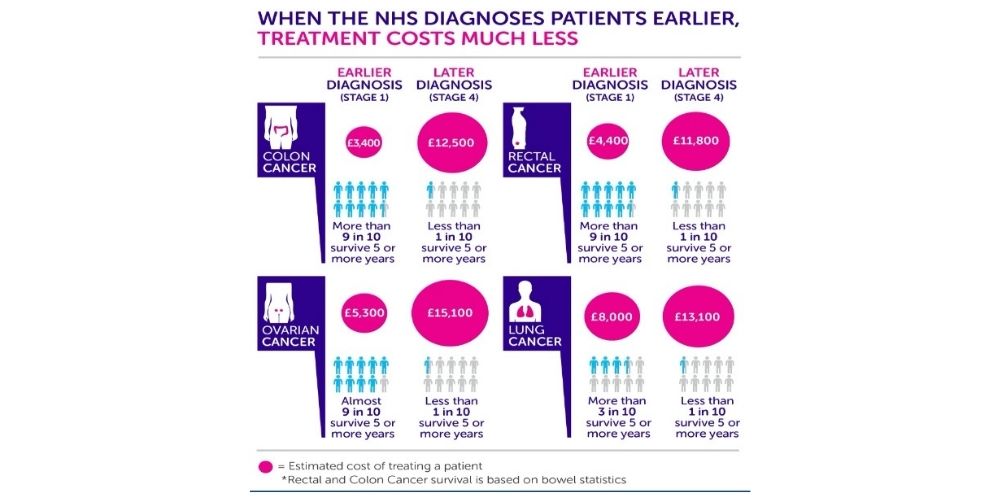
When patients are diagnosed earlier, treatment costs much less. Cancer Research UK prepared a report in 2014, “Saving lives, averting costs.” According to its calculations, back then a patient in stage I of colon cancer would cost the National Health Service on average £3,400. For the same patient, diagnosed at stage IV with the same cancer, it would be four times as much, around £12,500. That is just on the cost side. But looking at the survival rate, the difference is even more striking. If diagnosed early, at stage I, more than 9 out of 10 patients would survive five years or more, but at stage IV, less than 1 in 10 would. A similar picture applies to other cancers as well. In collaboration with the University of Cambridge, Cancer Research UK estimated that a 10% shift of patients from a late-stage presentation, stage III or IV, to early-stage diagnosis, would generate, in England alone, a £1 billion cost saving to the NHS over three years.
An OECD report, previously referred to by Dr. Muthu, revealed that about 20% of healthcare spending is currently being wasted on ineffective or inefficient interventions, and this could be even up to 40%, in certain healthcare situations. SPCC and AllCan are preparing a report at the moment, which will cover some of the aspects of efficiency vs inefficiency. Within cancer patient pathways, where are the most likely areas of ineffectiveness? Based on unpublished findings by the OECI, they are:
- Overtreatment
- Inefficiencies in care pathway integration
- Transfers of care between different institutions
- Poor internal communication, especially with supportive care disciplines
- Lack of community resources to support patients at the end of the acute treatment phase
- Poor data, or IT systems which do not cohere properly
Interestingly enough, through the experience of OECI, these days ineffectiveness is not so commonly found in the area of uniprofessional care decisions. Multidisciplinarity is well-established in the majority of cancers care settings, more in fact, because of the nature of cancer in terms of low adherence to medication that might affect other care conditions.
Good news – areas where OECI finds that inefficiencies are being conquered
OECI published a paper in Molecular Oncology in March 2021, “Analysing the attributes of Comprehensive Cancer Centres and Cancer Centres across Europe to identify key hallmarks”. Its findings of 40 cancer centres across Europe indicate that they all performed well in the areas of multidisciplinarity, pathway-based and patient-centred care, although the comprehensive cancer centres generally scored better. In particular, the use of MDT meetings for diagnosis and treatment recommendations, is now the norm in all centres. There are still some challenges in Central and Eastern Europe where multidisciplinary teams are not yet present in all cancers, and that t will be addressed in Europe’s Beating Cancer Plan and joint actions.
Methods for tackling the main inefficiencies
1) Overtreatment:
Clinical trials need to be established in dose de-escalation. Two ground-breaking Cambridge-led radiotherapy trials for high-risk and low-risk breast cancer patients demonstrated that radiotherapy doses can be reduced without affecting the efficacy for patients. Similar kinds of trials need to be replicated throughout cancers and modalities.
Despite the cost of genomic profiling, which should decrease in time, most clinicians would agree that much adjuvant chemotherapy is “scattergun”. And that is particularly true in certain forms of breast cancer. Whole-Genome and RNA sequencing can establish targeted populations and identify patients for whom therapies will not be effective. It is estimated that in certain types of breast cancer about 50% of chemotherapy is wasted or inefficient because we simply do not know, without genomic profiling, which patients will respond, and which will be resistant. Other forms of treatment optimization, including measuring cost/benefit need to be tackled. The European Organisation for Research and Treatment of Cancer (EORTC) is at the forefront of this, and the EU, as part of the Beating Cancer Plan, is about to establish a cancer medicines forum, focussing on treatment optimisation. Other indicators could also be measured, such as which therapies are being administered closely before death; we can look at quality and outcome measures, and we certainly should focus on patient reported outcomes and experience to tackle the huge issue of overtreatment.
2) Inefficiencies in care pathway integration:
Most of the issues are between primary and secondary care, with patients complaining about multiple visits to GPs. In the UK, the average general practitioner only sees between six and eight suspected cases of cancer per year, therefore organizations such as Macmillan Cancer Support and Cancer Research UK have provided and developed diagnostic algorithms for GPs to identify those patients who may have a conjunction of two or three symptoms, and immediately put them on what in England is called the two-week wait. There is reasonable evidence that once “in the secondary care system” waiting times are monitored and patients are tracked.
3) Transfers of care between different institutions are a cause of inefficiency, especially in complex cases (often inpatients). We need to deal with bed capacities, which in some health systems are very limited. For instance, the NHS in England has reduced its bed capacities. At the Cambridge Cancer Research Hospital, which treats more than 7,000 new patients a year, there are only 100 beds for adults, 100 inpatient beds in total. The capacity for transfers of care is limited by that one factor.
When a patient comes from a general hospital to a tertiary specialist centre, often there is a second reading of the radiology, because there are more specialist radiologists in the tertiary setting. It is not necessarily wrong, but there is something inherently inefficient within that particular transfer of care. Also, there needs to be good communication between hospitals.
This was the reason that in England, the first country to have tackled that in the late 1990s, cancer networks were established throughout, and patient pathways were painstakingly negotiated between care providers. Obviously, there were financial implications, but cancer by cancer, the patient pathways were reset, and specialist centres redefined for different cancers. This needs to happen in all health economies to tackle this particular inefficiency.
4) Poor internal communication, especially with supportive care disciplines. There are a number of ways to handle these inefficiencies. For instance, to involve appropriate supportive care disciplines in the MDT case meetings, rather than just referring to them afterwards; have joint clinics with supportive disciplines, head and neck counsel is a case in point, where swallow therapists and speech therapists are in the same clinic as the oncologists, getting involved at an early stage; have clear referral points into supportive care for each cancer pathway; those need to be supported by really good electronic holistic needs assessment processes. This could be done on an electronic device, with questions and answers before an outpatient appointment so that the patient can accurately communicate their own needs and priorities, which may be different from those of the clinicians managing them.
5) Lack of community resources to support patients at the end of the acute treatment phase.
This is a big issue in many health systems, and not an easy one to solve. But the first thing is
to have an established team in the hospital to manage the organisation of community care for discharged patients; that community team needs to be well resourced and integrated between different providers, who could be funded by the region or primary care, charities, or non-profit organizations; communication channels need to be clear and contacts for re-admission/acute oncology clearly understood; optimal communication should be ensured with patients and nurses, who can often be the best point of contact, and should be involved in the whole process.
6) Poor data, or IT systems which do not cohere properly
The solution could be a cancer network approach to data management and, even wider than that, a national approach. There are good examples of this in some Nordic countries, namely Sweden and Finland. Even if the hospitals have different electronic patient record systems, as is often the case, IT teams should work on systems interoperability, especially data mining and cohort data extraction. It is a hard and painstaking work, but it absolutely needed, as many members of MDTs cannot get the cohort data out of the system because the protocols have not been written. It is all there, in each individual electronic patient record, but to try and get an analysis of survival or quality of life, or even treatment trends, you have to go through each patient record or do a clinical audit. We also must not rely entirely on ICT, and use human case managers as well.

Other overall solutions for efficiency in patient pathways
There are also some overall solutions to implement. As already mentioned, a vital one is the human role of the case tracker, also called case manager or contact nurse, professionals who follow and monitor the patient, schedule tests and appointments, and make sure that the patient is presented to an MDT on time. They are extremely valuable. Those nurses should be involved in MDT meetings as well, so that they can hear and learn, and immediately take care of the patient pathway. This is common in Northern Europe, but not so much in Southern Europe. There could be a team to manage diagnostic scheduling of appointment prioritisation, making sure there is a one-stop-shop approach, which is so helpful for patients. There should be a failsafe IT method of monitoring waiting times at each point of the pathway; and a way to ensure that all patient pathways are clearly documented and understood by staff. Much of this falls into the realm of “process management” and could be learned from other industries.
Final essential ingredients for pathway effectiveness
An empowered and informed patient is going to make better decisions for their care. Effective team working of the integrated practice unit is vital. A small number of key performance indicators for management needs to be identified. Each MDT should have “quality circles”, perhaps twice a year, to review the cohort data from IT and identify the trends and the outcomes. Finally, compliance with international clinical guidelines in cancers must be reviewed.
The webinar online










